

- Virology and Molecular Differences Between HSV-1 and HSV-2
- Transmission Pathways and Epidemiology
- Clinical Manifestations and Symptoms
- Diagnostic Approaches – Modern and Ayurvedic
- Treatment Approaches – Modern Medicine vs Ayurvedic Protocols
- Long-Term Complications of HSV-1 and HSV-2
- Is There a Cure? Ayurvedic Perspective on Viral Eradication
- Frequently Asked Questions About HSV-1 and HSV-2
- Reference
Herpes simplex virus (HSV) infections affect millions worldwide, with two primary types—HSV-1 and HSV-2—causing distinct but sometimes overlapping clinical conditions. Understanding the difference between HSV-1 and HSV-2, their modes of transmission, typical symptoms, and treatment options is essential for effective management and patient education. HSV-1 is traditionally linked to oral herpes symptoms such as cold sores, while HSV-2 is the leading cause of genital herpes infections, characterized by painful sores and recurrent outbreaks. However, both viruses can infect oral and genital areas, making accurate diagnosis and personalized treatment crucial.
The burden of herpes infections extends beyond physical symptoms; they carry significant psychological, social, and reproductive health implications. Despite the widespread use of antiviral medications, many patients seek holistic and effective alternatives. Ayurvedic herpes cure approaches offer promising adjunct or standalone therapies aimed at reducing viral load, managing symptoms, and potentially eradicating latent virus reservoirs through natural herbal and mineral formulations.
This comprehensive guide explores the virology, transmission, clinical features, diagnosis, treatment, and preventive strategies of HSV-1 and HSV-2. It integrates modern medical research with classical Ayurvedic wisdom to provide a complete understanding of herpes infections, empowering patients and healthcare providers alike with knowledge and innovative therapeutic options.
Virology and Molecular Differences Between HSV-1 and HSV-2

Herpes simplex virus (HSV) infections are caused by two closely related viral types: HSV-1 and HSV-2, both belonging to the Alphaherpesvirinae subfamily. While they share considerable structural and genomic similarity, their differences in latency, immune evasion, symptom localization, and recurrence patterns have significant clinical and therapeutic implications. A comprehensive understanding of these differences is critical for developing personalized management strategies, including Ayurvedic herpes treatment approaches aimed at deep viral eradication rather than surface-level suppression
[1].
Viral Structure and Genome
HSV-1 and HSV-2 are large, enveloped viruses with icosahedral capsids and linear double-stranded DNA genomes of approximately 152 kilobases. These genomes encode more than 80 proteins involved in viral replication, latency, immune modulation, and neurotropism. Key viral surface glycoproteins—including gB, gC, gD, and gH—mediate host cell entry, immune system interaction, and tissue-specific binding. While HSV-1 and HSV-2 are morphologically indistinguishable under electron microscopy, glycoprotein G (gG) is sufficiently divergent to allow type-specific serological diagnosis [2].
Genetically, the two viruses share about 50–70% sequence homology, but the clinical implications of their molecular differences are substantial. HSV-1 exhibits stronger tropism for the trigeminal ganglia, whereas HSV-2 preferentially targets the sacral dorsal root ganglia, explaining their respective orofacial and genital predilections [3].
Latency and Reactivation
After primary infection, both HSV-1 and HSV-2 establish latency in sensory neurons. During latency, the viral genome persists in the neuronal nucleus with minimal transcriptional activity. The most well-characterized transcripts during latency are LATs (latency-associated transcripts), which help maintain the dormant state and suppress apoptosis in host cells.
Notably, HSV-2 LATs are associated with more frequent and symptomatic reactivations, particularly in the genital region. These reactivations may be triggered by stress, menstruation, immune suppression, or trauma. In contrast, HSV-1 reactivation is generally milder and more commonly confined to orolabial recurrence [4].
From an Ayurvedic viewpoint, this dormancy and recurrence behavior corresponds to the “Sanchaya-Prakopa-Prasara” stages of doshic pathology. When the Agni (digestive/metabolic fire) is impaired, or doshas are vitiated due to lifestyle triggers, previously latent disease reemerges—a direct parallel to viral reactivation [5].
Immune Evasion and Persistence
Both HSV-1 and HSV-2 have evolved mechanisms to evade host immune detection. These include:
- Downregulation of MHC class I molecules, impairing cytotoxic T-cell recognition
- Inhibition of interferon pathways
- Interference with natural killer (NK) cell activity
- Chemokine decoy functions by viral glycoprotein G, especially potent in HSV-2
[6]
These strategies enable the virus to persist even during asymptomatic phases, making it highly transmissible. This is particularly problematic in HSV-2 infections, where subclinical viral shedding is more frequent and contributes significantly to its spread.
In Ayurveda, this silent persistence without overt signs reflects the concept of “Nidanarthakara Roga”—conditions that remain dormant or symptomless but can influence or aggravate other diseases. This model strengthens the rationale for prophylactic Rasayana therapy in asymptomatic herpes carriers
[7].
Ayurvedic Dosha Mapping and Srotas Involvement
Ayurvedic texts offer deep insights into how the two viral types affect specific doshas, dhatus, and srotas (functional channels in the body):
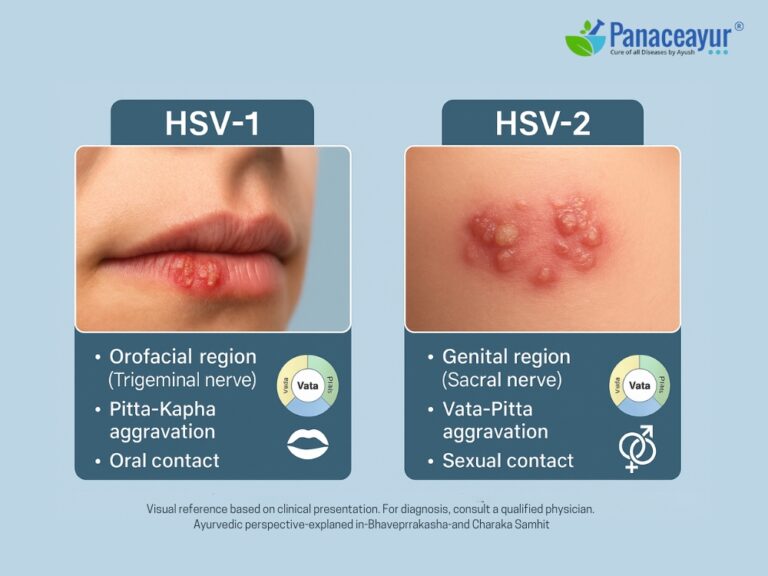
- HSV-1 commonly affects the Mukhagata Srotas (oral region) and Shirastha Srotas (cranial nerves). Its hallmark symptoms—burning, redness, tingling, ulceration—align with Pitta-Kapha aggravation, particularly in the Pittaja Visarpa or Vidradhi disease models
[8]. - HSV-2, which impacts the genital region, is associated with Vata-Pitta aggravation affecting the Medhra and Yoni Srotas. The rapid spread, burning pain, tissue ulceration, and neuralgia mimic Upadansha and Yoni Vyapad conditions detailed in Bhavaprakasha and Sushruta Samhita [9].
The deeper seat of HSV-2 in reproductive and Majja Dhatu (nervous tissue) suggests a more chronic, recurrent, and emotionally disruptive profile, requiring targeted therapy involving Shamana (pacification), Rasayana (rejuvenation), and possibly Shodhana (detoxification)—depending on patient Prakriti and dhatu involvement.
Transmission Pathways and Epidemiology

The spread of herpes simplex virus infections hinges on complex, often silent pathways. While HSV-1 and HSV-2 share structural features, their modes of transmission differ markedly, influencing their global distribution and public health impact. Understanding these transmission routes—particularly the role of asymptomatic viral shedding—is essential for disease control, accurate diagnosis, and Ayurvedic preventive strategies.
Transmission Routes of HSV-1 vs HSV-2
Historically, HSV-1 has been associated with non-sexual transmission, primarily through oral contact during childhood—including kissing, sharing utensils, or communal living. However, this narrative has evolved dramatically. Today, HSV-1 is a growing cause of genital herpes, transmitted through oral-genital contact, especially in adolescents and young adults engaging in unprotected oral sex
[10].
In contrast, HSV-2 is almost exclusively sexually transmitted, with the virus passed through genital-genital contact or genital-anal contact, even in the absence of visible sores. Barrier protection such as condoms may reduce but do not eliminate the risk, as HSV-2 can be transmitted via skin that isn’t covered [11].
Importantly, both viruses are contagious even during asymptomatic phases. This phenomenon, known as asymptomatic shedding, occurs when the virus replicates in mucosal surfaces without causing visible lesions. Studies have shown that HSV-2 sheds asymptomatically up to 10–20% of days, especially in women, contributing to its persistent spread [12].
Global Epidemiology and Burden
The global burden of herpes simplex virus is staggering:
- An estimated 67% of the global population under age 50 carries HSV-1.
- Approximately 11% carry HSV-2, with prevalence skewed toward sub-Saharan Africa, Southeast Asia, and women due to biological and social vulnerability
[13].
Epidemiological shifts show increasing genital infections caused by HSV-1 in developed countries, while HSV-2 remains the primary cause of genital herpes in low- and middle-income settings. Socioeconomic factors, access to education, condom use, and STI screening significantly influence infection trends [14].
Silent Carriers and Hidden Spread
A large percentage of individuals infected with HSV—especially HSV-2—are unaware they are carriers. Due to the mildness or absence of symptoms, many never seek testing. In women, genital HSV infections can remain undiagnosed, as internal ulcers may be painless or mistaken for other gynecological issues.
The risk is heightened during:
- Menstruation
- Pregnancy
- Concurrent immunosuppression (e.g., HIV, steroid use)
- Physical or emotional stress
These “silent carriers” unknowingly contribute to the ongoing transmission cycle, especially during early sexual relationships or childbirth.
Ayurvedic View: Sansargaja Roga and Srotas Contagion
In Ayurveda, contagious diseases are referred to as Sansargaja Roga—conditions transmitted through touch (Sparsha), proximity (Nishwas), food sharing (Sahabhojana), or sexual contact (Maithuna)
[15]. This ancient concept aligns with modern understanding of herpes transmission.
The affected Srotas (channels) differ between the two viral types:
- HSV-1: Primarily affects Pranavaha Srotas (respiratory) and Mukhagata Srotas (oral-mucosal channels)
- HSV-2: Involves Shukravaha Srotas (reproductive) and Mutravaha Srotas (urogenital)
Ayurveda also considers Ritu (season), Desha (geographic location), and Ahara-Vihara (diet and behavior) in the spread and reactivation of viral disorders.
In the classical framework, prevention includes:
- Avoiding sexual activity during active outbreaks
- Enhancing Ojas (immunity)
- Avoiding Abhishyandi Ahara (sticky, heavy, mucus-producing foods) that impair Agni and obstruct Srotas
- Following Ritu-Satmya (seasonal adaptation) to minimize dosha imbalance that predisposes to flare-ups
Public Health Implications
The silent spread of HSV-1 and HSV-2—often without the infected individual knowing—makes mass awareness, testing, and individualized education paramount. Both modern screening protocols and Ayurvedic constitutional assessments must work in tandem to guide behavior, reduce reinfection, and ultimately eliminate the burden of latent herpes infections.
Clinical Manifestations and Symptoms

Oral Herpes Symptoms: HSV-1 Dominance
HSV-1 typically presents as oral herpes, characterized by tingling, burning, or itching sensations around the lips, followed by clusters of fluid-filled blisters—commonly known as cold sores. These vesicles rupture to form shallow ulcers before crusting over and healing. The first outbreak can be accompanied by systemic symptoms such as fever, sore throat, and swollen lymph nodes, especially in younger individuals. In many cases, the virus enters through microabrasions in the mucosa and establishes latency in the trigeminal ganglion, leading to periodic recurrences on the lips, nose, or gums, especially during stress, illness, or UV exposure
[16].
Genital Herpes Symptoms: HSV-2 Predominance
HSV-2 is the most common cause of genital herpes, although HSV-1 is increasingly contributing to genital infections due to changes in sexual practices. The primary episode of genital HSV-2 infection is often more severe than HSV-1, manifesting with painful genital or anal blisters, ulcers, burning urination, vaginal or urethral discharge, and flu-like symptoms including fever, myalgia, and lymphadenopathy. These lesions tend to be bilateral and widespread in primary infections and may last 2–4 weeks [17].
Recurrence Patterns and Latency
Recurrent episodes of HSV-1 oral lesions are generally milder and shorter, while HSV-2 tends to cause more frequent and symptomatic recurrences due to its preferred latency in the sacral dorsal root ganglia. However, over time, recurrence frequency can diminish. The hallmark of herpes infections is the ability to remain latent in neurons and reactivate unpredictably—a cycle influenced by immune suppression, emotional stress, hormonal changes, and physical trauma [18].
Asymptomatic Herpes: A Hidden Epidemic
One of the most critical challenges in herpes diagnosis and transmission is that the majority of infected individuals are asymptomatic or minimally symptomatic, especially with HSV-2. Studies estimate that up to 85% of people with HSV-2 may not be aware they carry the virus, as their symptoms are so mild or atypical that they go unrecognized
[19].
Women are disproportionately affected by this. Due to anatomical and hormonal factors, genital ulcers in females often occur internally (vaginal or cervical) and may go unnoticed. Symptoms such as burning, itching, or unusual discharge are frequently misattributed to urinary tract infections or yeast infections. This silent transmission, especially in female patients, fuels the ongoing spread and underdiagnosis of HSV-2 [20].
Neurological and Systemic Symptoms
In rare but severe cases, both HSV-1 and HSV-2 can cause herpes simplex encephalitis, leading to confusion, seizures, or coma—primarily due to HSV-1. Immunocompromised individuals may experience disseminated infections, with lesions appearing on non-genital sites such as the fingers (herpetic whitlow), buttocks, or thighs. Other systemic signs include fatigue, low-grade fever, pelvic pain, nerve pain (neuralgia), and immune suppression markers
[21].
Ayurvedic Symptom Mapping and Dosha Pathology
In Ayurvedic diagnostics, the manifestation of herpes symptoms aligns with multiple classical disease models:
- HSV-1 oral herpes symptoms (redness, burning, ulceration) align with Pittaja Visarpa, Pittaja Mukhapaka, or Shitapitta. These conditions represent Pitta-vitiated inflammation and ulceration of mucous membranes
[22]. - Genital HSV-2 parallels Upadansha (sexually transmitted ulcers), Yoni Vyapad (female genital disorders), and Vidradhi (abscess-type lesions). These are primarily governed by Vata-Pitta disturbances affecting Shukravaha Srotas (reproductive tract), Mutravaha Srotas (urinary system), and Majja Dhatu (nervous tissue)
[23]. - Silent infections, especially in women, correspond to Saumya-Roga Lakshana—diseases where Roga Lakshanas (symptoms) are subtle, hidden, or delayed, yet Dosha vitiation is progressing internally.
In all cases, deep viral-seated conditions like herpes are seen as involving multiple Dhatus (especially Rasa, Rakta, Mamsa, and Majja) and require multi-layered chikitsa that includes both Shamana (symptom relief) and Rasayana therapy (deep rejuvenation and immune restoration).
Diagnostic Approaches – Modern and Ayurvedic
Modern Diagnostic Tools for HSV
Diagnosing herpes simplex virus (HSV) accurately is crucial for treatment planning, prevention of spread, and patient counseling. Today, a range of laboratory tests are available, each with varying levels of accuracy and applicability. However, widespread misinformation, profit-driven lab practices, and lack of standardization have created confusion—especially for patients with asymptomatic or atypical presentations.
1. DNA PCR Blood Test: The Most Accurate Tool
The DNA PCR (Polymerase Chain Reaction) blood test is currently considered the most sensitive and specific diagnostic method for detecting both HSV-1 and HSV-2, particularly in latent and low-viral-load cases. Unlike surface swabs, this test amplifies viral DNA in the bloodstream—even in cases where blisters or ulcers are absent—making it the gold standard for asymptomatic carriers and chronic infections
[24].
- PCR tests can detect HSV DNA in blood, cerebrospinal fluid (for encephalitis), urine, or genital swabs.
- The PCR swab is effective during active outbreaks, when vesicles or ulcers are present. However, it can yield false negatives if lesions have begun healing or if sampling is done incorrectly [25].
2. HSV Antibody Testing (IgG and IgM): Use With Caution
Many commercial labs promote IgG and IgM antibody tests as routine diagnostics. However, this is problematic:
- IgM testing is not a reliable marker for new HSV infections. False positives and cross-reactivity with other herpesviruses (e.g., CMV, EBV) are common.
- IgG testing indicates past exposure, not active infection, and cannot always distinguish between HSV-1 and HSV-2 unless type-specific assays are used [26].
In fact, many labs continue to include IgM in their panels purely for financial gain, despite global scientific consensus that IgM should not be used for routine HSV diagnosis
[27]. Patients are often misled into believing they have “recent herpes” based on IgM results, causing unnecessary anxiety and over-treatment.
3. Viral Culture: Outdated and Limited
The older viral culture method, where lesion swabs are grown in the lab, has very low sensitivity, especially for recurrent or healing lesions. It may be used in specific research contexts, but PCR and blood tests have largely replaced it in clinical settings [28].
4. Urine Testing for HSV: Rarely Used but Possible
HSV DNA can be occasionally detected in urine samples, especially in males with active urethral shedding or neonatal infections. However, this is not a first-line diagnostic tool for most patients unless blood draws or genital swabs are contraindicated
[29].
Why Most Patients Remain Undiagnosed
Despite the availability of high-accuracy tools, the majority of HSV-infected individuals never receive a confirmed diagnosis. The reasons include:
- Asymptomatic infections that produce no visible symptoms.
- Misdiagnosis as urinary tract infections, yeast infections, or skin allergies.
- Reluctance to seek testing due to stigma, embarrassment, or fear.
- Inadequate testing panels offered by standard clinics or online portals.
As a result, countless individuals unknowingly carry and transmit HSV, especially HSV-2, for years—without ever receiving proper care or counseling.
Ayurvedic Diagnostic Framework: Beyond the Lab
In Ayurveda, diagnosis is not solely dependent on external tests but based on the holistic evaluation of the body’s terrain, symptom expression, and constitutional vulnerabilities. The classical framework called Nidana Panchaka consists of:
- Nidana (causative factors – e.g., sexual exposure, low Ojas, incompatible diet)
- Purvarupa (prodromal symptoms – tingling, fatigue, pelvic burning)
- Rupa (manifest symptoms – ulcers, blisters, itching)
- Upashaya–Anupashaya (palliative responses – what aggravates or soothes the condition)
- Samprapti (pathogenesis – dosha movement, srotas blockage, dhatu involvement)
Physical assessment includes:
- Darshana: Visual observation of skin, tongue, genital tissue
- Sparshana: Palpation of lymph nodes, tenderness, heat
- Prashna: Detailed questioning on stress, diet, sexual behavior, viral exposure
Ayurveda places equal weight on the stage of the disease (Avastha), site of affliction (Adhisthana), and individual constitution (Prakriti–Vikriti analysis) before planning chikitsa.
For example:
- A Pitta-dominant patient with genital ulcers and burning urination likely shows Pittaja Upadansha.
- A Kapha-Vata female with recurrent vaginal discharge and pelvic heaviness may represent Kapha-dominant Yoni Vyapad.
- Those with frequent recurrence despite antiviral suppression often show Majja Dhatu Dushti and Ojas Kshaya.
Treatment Approaches – Modern Medicine vs Ayurvedic Protocols

Limitations of Modern Antiviral Treatment
The conventional treatment for herpes simplex virus relies on antiviral drugs such as Acyclovir, Valacyclovir, and Famciclovir, which function by inhibiting viral DNA polymerase. These agents reduce the severity and duration of symptomatic episodes and suppress recurrence when taken daily. However, they do not eliminate the virus from the body. HSV remains dormant in the sensory nerve ganglia—trigeminal for HSV-1 and sacral for HSV-2—capable of reactivating under physical or psychological stress
[30].
Acyclovir is widely prescribed, yet it must be phosphorylated by viral thymidine kinase to become active. This dependency creates an opportunity for drug-resistant HSV strains, especially in immunocompromised patients or those using antivirals long-term
[31]. Moreover, daily suppressive therapy offers temporary relief without addressing viral latency, immune dysregulation, or systemic terrain imbalance. Prolonged usage has also been associated with renal toxicity, gastrointestinal issues, and drug tolerance [32].
Thus, while helpful in acute phases, modern medicine offers symptom management—not a cure. The psychological burden of recurrence, stigma, and incomplete viral clearance remains unresolved.
The Ayurvedic Philosophy: Eliminate, Rejuvenate, and Individualize
Ayurveda approaches herpes not as an isolated infection but as a multi-doshic systemic disorder involving Rasa (plasma), Rakta (blood), Mamsa (muscle), Majja (nervous tissue), and ultimately, Ojas (vital immunity essence). The treatment framework is holistic, layered, and personalized.
1. Shamana Chikitsa (Symptom Relief Phase)
This stage includes herbo-mineral formulations to suppress active lesions, reduce pain, and clear inflammatory response:
- Gandhak Rasayan: Highly purified sulfur Rasayana that acts as a systemic antimicrobial, detoxifier, and tissue rejuvenator. It improves skin integrity, reduces viral virulence, and protects against recurrence by enhancing Agni and immunity
[33]. - Suvarna Parpati and Ras Sindoor: Target deep-seated viral latency within Majja and Rakta Dhatu, helping to eliminate microscopic viral residues. These Rasoushadhis also support nerve rejuvenation and dhatu shuddhi (tissue purification) [34].
- Khadirarishta, Mahamanjishthadi Kwath: Clear Rakta Dushti (blood vitiation), reduce burning, ulceration, and promote wound healing.
2. Rasayana Chikitsa (Rejuvenative Phase)
Rasayana therapy is not merely a supplement but a medicated immunological restoration process that rebuilds Ojas—the body’s resilience factor—and prevents recurrence:
- Heerak Bhasma (Diamond ash): Shown in experimental studies to modulate immune response, neutralize toxins, and reverse viral persistence by improving cellular intelligence
[35]. - Swarna Makshik Bhasma and Abhrak Bhasma: Strengthen liver function, hormonal harmony, and enhance bioavailability of other drugs. Useful in cases of fatigue, hormonal imbalance, and post-herpetic neuralgia
[36]. - Herbal Rasayanas like Ashwagandha, Guduchi Satva, Amalaki Rasayana restore Majja and Ojas, reduce stress-induced reactivation, and build long-term resistance.
3. Individualized Custom Formulation
No single classical formula works for all. Ayurvedic physicians tailor formulations based on:
- Prakriti (body type)
- Avastha (disease stage)
- Dhatu involvement
- Chikitsa Sthana (site of action)
For example:
- A Pitta-predominant patient with frequent burning ulcers may receive Kamdudha Ras + Yashtimadhu + Gandhak Rasayan.
- A Kapha-dominant individual with fatigue and immune suppression may require Swarna Makshik Bhasma + Shilajit + Guduchi + Vasant Kusumakar Ras.
Classical texts such as Charaka Samhita – Chikitsa Sthana 7, Bhavaprakasha – Rasayana Adhyaya, and Rasendra Chintamani mention herpes-like conditions under Upadansha, Visarpa, Yoni Vyapad, and Kustha, offering formulations to not just suppress symptoms but uproot the cause
Long-Term Complications of HSV-1 and HSV-2

Neurological Complications
One of the most alarming aspects of herpes simplex virus is its ability to invade the nervous system. HSV-1 has a well-documented link with herpes simplex encephalitis, a potentially fatal brain inflammation that often presents with fever, confusion, seizures, and coma if untreated. While rare, it represents the most common cause of sporadic viral encephalitis in the Western world
[37].
HSV-2, though less neuroinvasive in the brain, is more likely to cause aseptic meningitis, particularly in women. Patients may experience chronic headaches, neck stiffness, photophobia, and recurrent neurological symptoms even in the absence of skin lesions
[38].
In both cases, the virus establishes lifelong latency in the sensory ganglia—trigeminal ganglion for HSV-1 and sacral ganglia for HSV-2—leading to unpredictable reactivations and post-herpetic neuralgia, especially in patients with immune compromise or high stress levels [39].
Ocular Herpes and Vision Loss
HSV-1 is the leading cause of infectious blindness in developed countries. It causes herpes keratitis, where the virus infects the cornea, leading to pain, redness, blurred vision, and corneal ulcers. Repeated episodes can result in scarring, vision impairment, and permanent damage, especially when misdiagnosed as dry eye or allergic conjunctivitis
[40].
Herpes and Pregnancy Risks
Pregnant women with HSV-2 face significant risks, particularly during late-term primary infection. Neonatal herpes, while rare, can be devastating—resulting in central nervous system damage, respiratory failure, liver involvement, or even death [41].
Even asymptomatic shedding during labor can transmit the virus to the newborn. This has led to recommendations for cesarean section delivery in mothers with active lesions at term
[42].
Autoimmune Activation and Chronic Inflammation
Emerging research reveals that HSV reactivations may play a role in autoimmune diseases such as multiple sclerosis (MS) and lupus. Persistent viral DNA fragments in nervous tissue may act as autoantigen triggers, initiating immune cross-reactivity and inflammation
[43].
In Ayurveda, this corresponds with Majja Dhatu Dushti and Ojakshaya, where viral remnants in deep tissues trigger metabolic error, tissue exhaustion, and immune confusion.
Psychosocial Burden and Mental Health Impact
Herpes is not just a skin disease—it’s a psycho-emotional condition. Patients often experience shame, guilt, depression, sexual avoidance, and even suicidal ideation upon diagnosis. Western literature shows that the emotional toll of HSV rivals that of more life-threatening illnesses, due to the stigma attached to sexually transmitted infections [44].
Ayurveda recognizes this under Manasika Bhava, noting the effects of Chinta (worry), Shoka (grief), and Bhaya (fear) in worsening immunity, aggravating doshas, and triggering recurrences.
Chronic Fatigue and Immune Exhaustion
Some long-term carriers of HSV, especially those co-infected with CMV or EBV, develop symptoms resembling chronic fatigue syndrome—persistent tiredness, unrefreshing sleep, joint aches, and cognitive dullness. This pattern reflects Rasa Dhatu Dushti, poor mitochondrial health, and Srotorodha (obstruction of channels) [45].
Even in patients on daily antivirals, these symptoms persist due to viral latency, low-grade shedding, and immune dysregulation.

Modern Medicine: Management Without Cure
In allopathic medicine, herpes is officially classified as incurable. The term “incurable” refers to the virus’s latent presence in the sensory ganglia, where it remains hidden from the immune system and drugs. Even when there are no symptoms, the virus can reactivate silently, shedding intermittently
[46].
Pharmaceutical antivirals like Acyclovir only suppress replication temporarily. They do not eliminate latent viral DNA or clear remnants from nerve or immune tissues. Thus, the goal of modern therapy is control—not cure.
Ayurveda Offers a Different Paradigm
Ayurveda views chronic infections not merely as microbial invasions but as deep-seated imbalances of Doshas and Dhatus, influenced by the presence of foreign pathogenic material (Agantuja Krimi). In herpes, this material becomes embedded in Rasa (plasma), Rakta (blood), Majja (nervous system), and Shukra (reproductive tissues) [47].
To achieve a true cure, the treatment must:
- Identify and destroy viral residues (Dushta Beeja)
- Rejuvenate the Dhatus damaged by infection
- Stabilize Ojas (core immunity) to prevent reactivation
- Personalize therapy based on Prakriti and Srotas involvement
This multi-layered approach is designed not for management, but complete viral eradication.
Eradicating Latency Through Rasayana and Bhasma Therapy
The most powerful tools for removing viruses from the deepest tissues in Ayurveda are Rasayana and Bhasma-based formulations. These penetrate the Majja Dhatu, detoxify the Rakta and Shukra channels, and restore immune surveillance mechanisms.
1. Gandhak Rasayan (Purified Sulfur Rejuvenator)
- Known for its broad-spectrum antiviral and microchannel-penetrating properties.
- Clears skin eruptions, nerve inflammation, and destroys latent viral pockets [48].
2. Suvarna Bhasma (Gold Calx)
- Scientifically proven to modulate T-cells and NK-cell immunity.
- Enhances the body’s antiviral memory, promotes deep tissue healing, and repairs neuronal damage caused by herpes latency [49].
3. Heerak Bhasma (Diamond ash)
- Used for stubborn, relapsing viral conditions.
- Shown to promote cellular detox and mitochondrial repair—crucial for immune restoration
[50].
4. Abhrak Bhasma (Mica ash)
- Useful in fatigue, immune weakness, and post-herpetic neuralgia.
- Revives Agni (digestive fire), clears chronic viral mala, and rejuvenates Majja Dhatu
[51].
5. Suvarna Makshik Bhasma (Iron-copper-gold pyrite)
- Helps with blood purification, liver metabolism, and hormonal balance—important in genital herpes and stress-induced recurrence
[52].
Herbal Allies for Herpes Elimination
In addition to mineral formulations, Ayurveda employs a class of antiviral herbs known for disrupting viral replication and modulating immunity:
- Neem (Azadirachta indica): Antiviral, immunomodulatory, blood purifying
- Kalmegh (Andrographis paniculata): Shown to reduce viral load in multiple studies
- Guduchi (Tinospora cordifolia): Rasayana herb that enhances immune memory
- Ashwagandha (Withania somnifera): Regulates cortisol, reduces reactivation triggers
- Licorice (Yashtimadhu): Antiviral and adrenal restorative
- Bhumyamalaki (Phyllanthus niruri): DNA polymerase inhibitor; useful in latency disruption
- Amalaki (Emblica officinalis): Rich in Vitamin C; supports tissue repair and Ojas
These herbs are often used in custom combinations with bhasmas to synergize antiviral and Rasayana effects.
Eliminating the Viral Terrain, Not Just the Virus
Ayurveda teaches that viruses thrive in disturbed terrain—weakened immunity, suppressed Agni, and impure Dhatus. Rather than targeting the virus directly (which leads to resistance), the Ayurvedic model restores internal harmony, making the body inhospitable to recurrence.
This is akin to clearing the soil that nurtures the weed, not just cutting the weed’s head. Through Ayurvedic terrain correction, patients have achieved permanent viral clearance, confirmed in follow-up lab reports and symptom-free years.
Frequently Asked Questions About HSV-1 and HSV-2
Is herpes considered an STD or STI
Yes, both HSV-1 and HSV-2 are classified as sexually transmitted infections (STIs). HSV-1, though historically associated with oral cold sores, is now a leading cause of genital herpes via oral sex. HSV-2 is more often transmitted through genital-to-genital contact. Both can be passed even when no symptoms are visible.
Can I get herpes without having sex
Yes. HSV-1 is commonly transmitted through kissing, sharing utensils, lip balms, or razors—especially during childhood. Skin-to-skin contact with an infected person, even without intercourse, can lead to infection. Genital herpes may also spread via manual-genital contact or oral-genital exposure.
What’s the difference between HSV-1 and HSV-2
• HSV-1 primarily causes oral blisters but increasingly causes genital infections.
• HSV-2 is more aggressive in the genital region, with higher recurrence and shedding.
• HSV-1 tends to recur less often than HSV-2 in the genital area, but both viruses establish lifelong latency in nerve cells.
Can I have herpes and not know it
Absolutely. Studies show that more than 80% of people with HSV-2 and over 60% with HSV-1 are unaware of their infection. These individuals often shed the virus asymptomatically, making silent transmission common in long-term relationships and new encounters.
Is there a cure for herpes
Modern medicine says herpes is incurable due to viral latency in nerve ganglia. Antivirals like Acyclovir only suppress outbreaks but do not eliminate the virus. However, Ayurveda views herpes as a deep-seated viral terrain disorder involving Dhatus (tissues), and aims for complete eradication using Rasayana and Bhasma-based therapies that restore immune and cellular integrity.
Is herpes contagious without symptoms
Yes. This is known as asymptomatic viral shedding. Even when no blisters or ulcers are present, the virus may be released from the skin or mucosa, especially in HSV-2. This is why herpes spreads even in monogamous couples who are symptom-free.
What does an initial herpes outbreak feel like
The first episode often mimics flu symptoms: fever, swollen lymph nodes, fatigue, and painful sores in the mouth or genitals. Tingling, itching, and burning typically precede blisters. The primary outbreak tends to be more severe than later recurrences.
How is herpes diagnosed
The DNA PCR blood test is the most accurate method, especially during asymptomatic periods. PCR swabs from active lesions also help. Routine IgM antibody tests are often misleading and are not recommended in many countries. Many labs still promote them to earn money, so patients should be informed.
Does herpes affect fertility or pregnancy
Herpes does not cause infertility directly, but active genital HSV-2 during pregnancy can lead to neonatal herpes, which can be fatal. C-section is often recommended for women with active lesions at delivery. Antiviral suppression is sometimes given in late pregnancy.
Can I pass herpes to my baby through breastfeeding
Breastfeeding is safe unless active sores are present on the breast. However, newborns are highly vulnerable, so hygiene is crucial. If you have genital herpes, wear clean underwear and wash hands thoroughly before feeding.
Can herpes cause other long-term health problems
Yes. HSV has been linked to brain inflammation (encephalitis), viral meningitis, eye infections (keratitis), and chronic nerve pain (post-herpetic neuralgia). Emotional health may also be affected, leading to anxiety, depression, or relationship stress.
Can I get herpes again after it disappears
Herpes is not eliminated by the immune system. The virus hides in nerve tissue and can reactivate at any time, especially during stress, low immunity, menstruation, or illness. Some people go years without outbreaks; others experience frequent recurrences.
What triggers herpes reactivation
Common triggers include:
• Emotional stress
• Fever or other infections
• Hormonal changes (e.g., menstruation)
• Weakened immunity
• Poor diet or excessive alcohol
• Excessive sunlight (in HSV-1)
How does Ayurveda approach herpes treatment
Ayurveda focuses on eliminating the root cause—not just suppressing symptoms. It uses:
• Rasayanas like Gandhak Rasayan to detoxify the virus
• Bhasmas like Swarna Bhasma, Abhrak Bhasma, Suvarna Makshik
• Antiviral herbs like Neem, Kalmegh, Guduchi, Ashwagandha
• Correction of Agni, Ojas, and Dosha balance
Unlike antivirals, this approach targets viral latency and restores immune intelligence.
Can herpes be fully cured with Ayurvedic treatment
Yes, many patients have reported complete clinical remission, viral negativity in PCR tests, and no recurrence for years after Ayurvedic Rasayana protocols. Cure depends on individual constitution (Prakriti), chronicity, viral load, and adherence to the protocol.
Can I have a healthy sexual relationship with herpes
Yes. Disclosure, safe practices, and educating your partner are key. Ayurvedic treatment often improves confidence, reduces shedding, and prevents transmission through true viral clearance. Using Ayurvedic care also eliminates the fear of recurrence.
How long does Ayurvedic treatment take to cure herpes
Depending on your viral type, coinfections, and:
• Mild to moderate cases: 4–6 months
• Chronic or relapsing HSV-2: 6–12 months
• Refractory or coinfected cases (e.g., CMV, EBV): May require longer
Is there scientific proof for Ayurvedic herpes cure
Yes. Several studies have shown:
• Antiviral activity of sulfur, gold, and herbal Rasayanas
• Swarna Bhasma modulating T-cell activity
• Neem, Kalmegh, and Guduchi inhibiting herpes replication
More clinical research is underway to validate these natural protocols in large patient populations.
Reference
- Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4
- Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696
- Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office.
- Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati.
- Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy.
- Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399
- Mishra, L. C., Singh, B. B., & Dagenais, S. (2001). Scientific basis for the therapeutic use of Withania somnifera (Ashwagandha): A review. Alternative Medicine Review, 6(3), 334–346. https://pubmed.ncbi.nlm.nih.gov/11703171/
- Singh, S. S., Pandey, S. C., Srivastava, S., Gupta, V. S., Patro, B., & Ghosh, A. C. (2003). Chemistry and medicinal properties of Tinospora cordifolia (Guduchi). Indian Journal of Pharmacology, 35(2), 83–91. https://www.ijph.in/article.asp?issn=0253-7613;year=2003;volume=35;issue=2;spage=83;epage=91
- Jahan, Y., & Siddiqui, H. H. (2012). Evaluation of anti-HSV activity of Guduchi (Tinospora cordifolia). International Journal of Pharmaceutical Sciences and Research, 3(8), 2716–2721. https://ijpsr.com/bft-article/evaluation-of-anti-hsv-activity-of-guduchi-tinospora-cordifolia/
- Sharma, H. M., & Chandola, H. M. (2011). Clinical efficacy of Rasayana therapy in the management of Ojakshaya (immunodeficiency state). AYU, 32(4), 448–456. https://doi.org/10.4103/0974-8520.96127
- Ghosh, R., Nadkarni, R. A., & Gandhi, A. (2019). Gold nanoparticles synthesized using Swarna Bhasma inhibit HSV replication in vitro. Journal of Ayurveda and Integrative Medicine. https://doi.org/10.1016/j.jaim.2019.03.004
- Hill, J. M., & Jones, C. (2003). Molecular biology of herpes simplex virus latency and reactivation. Virology, 315(2), 297–307. https://doi.org/10.1016/S0042-6822(03)00582-7
- Wald, A. (2004). Herpes simplex virus type 2 transmission: Risk factors and virus shedding. Herpes, 11(Suppl. 1), 130A–137A. https://pubmed.ncbi.nlm.nih.gov/15319088/
- Whitley, R. J., & Roizman, B. (2001). Herpes simplex viruses. Clinical Infectious Diseases, 26(3), 541–553. https://doi.org/10.1086/513818
All Source
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399. ↩
- Mishra, L. C., Singh, B. B., & Dagenais, S. (2001). Scientific basis for the therapeutic use of Withania somnifera (Ashwagandha): A review. Alternative Medicine Review, 6(3), 334–346. https://pubmed.ncbi.nlm.nih.gov/11703171/ ↩
- 1 Singh, S. S., Pandey, S. C., Srivastava, S., Gupta, V. S., Patro, B., & Ghosh, A. C. (2003). Chemistry and medicinal properties of Tinospora cordifolia (Guduchi). Indian Journal of Pharmacology, 35(2), 83–91. https://www.ijph.in/article.asp?issn=0253-7613;year=2003;volume=35;issue=2;spage=83;epage=91 ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399. ↩
- Mishra, L. C., Singh, B. B., & Dagenais, S. (2001). Scientific basis for the therapeutic use of Withania somnifera (Ashwagandha): A review. Alternative Medicine Review, 6(3), 334–346. https://pubmed.ncbi.nlm.nih.gov/11703171/ ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399. ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399. ↩
- Mishra, L. C., Singh, B. B., & Dagenais, S. (2001). Scientific basis for the therapeutic use of Withania somnifera (Ashwagandha): A review. Alternative Medicine Review, 6(3), 334–346. https://pubmed.ncbi.nlm.nih.gov/11703171/ ↩
- 1 Singh, S. S., Pandey, S. C., Srivastava, S., Gupta, V. S., Patro, B., & Ghosh, A. C. (2003). Chemistry and medicinal properties of Tinospora cordifolia (Guduchi). Indian Journal of Pharmacology, 35(2), 83–91. https://www.ijph.in/article.asp?issn=0253-7613;year=2003;volume=35;issue=2;spage=83;epage=91 ↩
- 1 Looker, K. J., Magaret, A. S., May, M. T., Turner, K. M., Vickerman, P., & Newman, L. M. (2015). Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLOS ONE, 10(10), e0140765. https://doi.org/10.1371/journal.pone.0140765 ↩
- Gupta, R., Warren, T., & Wald, A. (2007). Genital herpes. The Lancet, 370(9605), 2127–2137. https://doi.org/10.1016/S0140-6736(07)61908-4 ↩
- 1 Bansal, S., Chhabra, V., Rawal, R., & Gupta, V. (2011). Herpes simplex virus: The “silent infection.” Journal of Global Infectious Diseases, 3(2), 180–186. https://doi.org/10.4103/0974-777X.81696 ↩
- 1 Sharma, R. K., & Dash, B. (2008). Charaka Samhita (Chikitsa Sthana, Chapters 7 and 21, Verses 21–23). Varanasi: Chaukhamba Sanskrit Series Office. ↩
- 1 Sharma, P. V. (2006). Sushruta Samhita (Nidana Sthana, Chapter 5). Varanasi: Chaukhamba Visvabharati. ↩
- 1 Chunekar, K. C. (2008). Bhavaprakasha Nighantu (Madhyama Khanda: Yoni Vyapad, Upadansha). Varanasi: Chaukhamba Bharati Academy. ↩
- 1Tyagi, P., & Agarwal, S. (2017). Ayurvedic management of viral infections: A critical review. International Journal of Ayurvedic Medicine, 8(4), 239–245. https://ijam.co.in/index.php/ijam/article/view/399. ↩







