

- The Invisible Battlefield of Latency
- HIV Latency in Modern Science
- Ayurveda’s Latency Doctrine
- Mapping Ayurvedic Pathophysiology to HIV Reservoirs
- Purification Strategies in Ayurveda: Reaching the Root
- Purification Strategies in Ayurveda: Reaching the Root
- Scientific Parallels: Epigenetics, Immunotherapy, and Dhatu Cleansing
- Appendix
- References
The Invisible Battlefield of Latency
In the ongoing war against HIV, modern medicine has achieved remarkable victories. Combination antiretroviral therapy (ART) can reduce plasma viral load to undetectable levels, prevent transmission, and extend life expectancy to near-normal ranges. However, despite decades of pharmaceutical advancement, one critical front remains unconquered: latent HIV reservoirs—silent, inaccessible vaults where the virus hides, evades detection, and re-emerges when treatment stops. [1]
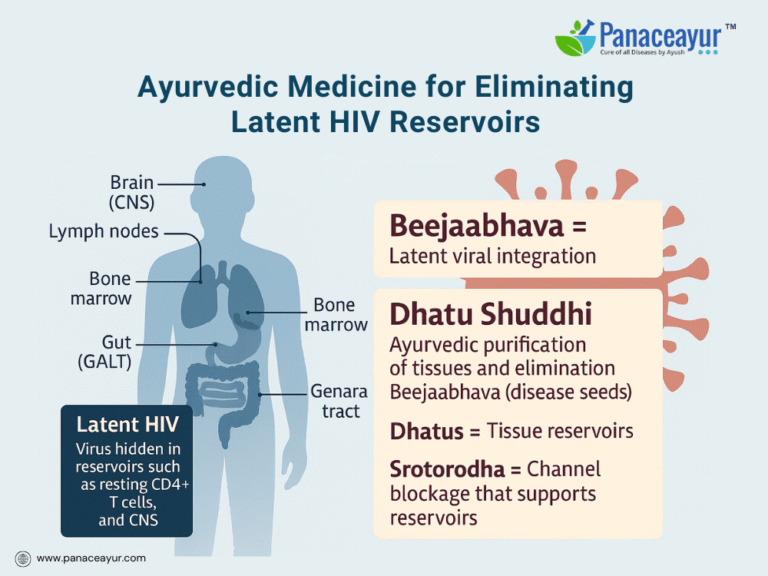
These latent reservoirs consist primarily of resting CD4+ T cells, monocytes/macrophages, and tissue-resident cells in organs such as the lymph nodes, gut-associated lymphoid tissue (GALT), bone marrow, brain (microglia), and genital tract. Within these anatomical sanctuaries, the virus integrates its genome into the host’s DNA, entering a transcriptionally silent state. Because the virus produces no proteins, it becomes invisible to both cytotoxic T lymphocytes and pharmaceutical inhibitors. [2]
This latency is the cornerstone of viral persistence. When ART is discontinued, HIV rapidly rebounds from these hidden sanctuaries—a phenomenon that has made eradication elusive and lifelong treatment necessary. [3] For the modern virologist, the quest to break this latency is now the “final frontier” of HIV cure research.
Yet while pharmaceutical science focuses on shocking and killing latent virus with latency-reversing agents (LRAs), Ayurveda takes a different path. It doesn’t attempt to forcibly awaken the virus. Instead, it aims to dismantle the internal environment—the biological and energetic terrain—that allows latency to persist.
This terrain-centric view is rooted in the classical Ayurvedic concept of Beejabhava Dosha, described in Charaka Samhita (Sharira Sthana 3/17), which speaks of the latent “seed” of disease lying hidden in the body until conditions favor its expression. [4] HIV, from this lens, is not merely a pathogen but a seed-like memory of disease embedded in weakened or obstructed tissues (Dhatus) and carried forward through disturbed microchannels (Srotas).
In biomedical terms, this can be compared to a genetic landmine: the viral genome sits silently in immune cells, waiting to be triggered by inflammation, hormonal imbalance, or immune activation. Similarly, Ayurveda views the Beejabhava Dosha as inert until activated by vitiated Doshas (Vata, Pitta, Kapha) or external stressors. [5]
Importantly, Ayurveda does not seek to destroy this seed through force. It seeks to alter the soil—to purify the Dhatus, open the blocked Srotas, and reawaken Agni (metabolic intelligence), so the internal terrain no longer supports viral latency. Just as a dormant seed cannot sprout in sterile, unfavorable soil, a purified body resists viral reactivation.
This is a sophisticated systems biology model. Instead of chasing the virus in hiding, Ayurveda neutralizes the environment that enables dormancy and recurrence.

The goal is not suppression, but disarmament. Not chemical inhibition, but cellular cleansing and metabolic realignment.
In the upcoming sections, we’ll explore how HIV latency works anatomically and genetically, how the ancient concept of Beejabhava aligns with modern virology, how Dhatus and Srotas serve as viral sanctuaries, and how purification therapies can systemically break this pattern of reactivation.
This is the conversation often missing in HIV treatment—not just controlling the virus, but changing the internal reality that allows it to persist.
HIV Latency in Modern Science

The central challenge in curing HIV today lies not in controlling its replication, but in eliminating its ability to hide. While antiretroviral therapy (ART) effectively suppresses the virus in the bloodstream, it cannot touch the silent form of HIV embedded within the body’s tissues. This phenomenon, known as HIV latency, refers to the virus’s ability to integrate its genetic material into the host genome of immune cells—particularly resting memory CD4+ T cells—without producing viral proteins. In this dormant state, HIV becomes immunologically invisible and pharmacologically unreachable.[6]
Latency is not confined to isolated cells; it is anchored in specific anatomical zones known as viral reservoirs. These reservoirs include the lymph nodes, gut-associated lymphoid tissue (GALT), central nervous system (CNS), bone marrow, male genital tract, spleen, liver, and even adipose tissue. In each of these sites, the virus finds safe harbor within long-lived immune cells or tissue-resident macrophages. These cells retain the proviral genome and serve as biological vaults, capable of reigniting infection when ART is stopped or immune surveillance weakens. [7]
What makes these sites particularly formidable is their combination of structural protection, immune privilege, and metabolic insulation. For instance, the blood–brain barrier restricts drug penetration into the CNS, and fibrotic changes in lymphoid tissue hinder immune access. Meanwhile, within the gut and bone marrow, HIV persists in relatively quiescent immune cells that are less likely to present viral antigens. ART does not penetrate these microenvironments effectively, and thus cannot eliminate the virus residing there. [8]
Modern medicine has attempted to confront this challenge with two major strategies: “shock and kill,” and “block and lock.” The first approach aims to awaken latent HIV using pharmacological agents like histone deacetylase inhibitors or TLR agonists, followed by cytotoxic therapies or immune clearance. However, this strategy has often led to systemic inflammation, partial reactivation, or immune escape. The second approach, “block and lock,” aims to silence HIV indefinitely by reinforcing transcriptional latency through gene-silencing technologies. Although promising in theory, it remains in the early experimental phase, and questions remain about the long-term safety of manipulating gene expression in host cells. [9]
Compounding these challenges is the virus’s use of epigenetic suppression to maintain latency. Integrated HIV is often found associated with heterochromatin regions, wrapped in repressive histone modifications and DNA methylation, and devoid of necessary transcriptional activators. This not only shields the virus from detection but also makes it extremely difficult to awaken fully and uniformly. Moreover, the immune cells responsible for eliminating infected cells, especially cytotoxic T lymphocytes, often display exhaustion markers such as PD-1, TIM-3, and LAG-3, further reducing their effectiveness in clearing the reactivated virus. [10]
The few cases where HIV has been functionally cured, such as the Berlin and London patients, involved stem cell transplantation with CCR5-Δ32 mutation donors—procedures that are risky, expensive, and not scalable to the broader patient population. These exceptions, while scientifically inspiring, highlight the absence of a universally applicable solution in current biomedical practice. [11]
All of this reveals a deeper truth: HIV latency is not merely a virological trick, but a systemic condition—rooted in immune dysfunction, anatomical shielding, and a disturbed internal environment. In many ways, the virus thrives not because it is strong, but because the host terrain allows it to survive undisturbed.
Here is where Ayurveda offers a paradigm shift. It does not attempt to attack the virus directly but instead focuses on restoring the health and purity of the body’s internal tissues. Through a conceptually profound yet clinically actionable framework, Ayurveda describes how the latent seed of disease can be eliminated by cleansing the body’s subtle tissues, improving immune intelligence, and restoring systemic harmony. In the next section, we explore this doctrine in detail through the lens of Beejabhava Dosha—a concept that may offer a new way of understanding HIV latency itself.
Ayurveda’s Latency Doctrine

In classical Ayurveda, the root of chronic and recurring diseases is not always visible at the surface level of symptoms or blood parameters. The ancient seers recognized that certain diseases remain latent—unmanifested yet potent—until the right conditions allow them to emerge. This concept is known as Beejabhava Dosha, literally translating to “the doshic seed of disease.” It is described in Charaka Samhita, Sharira Sthana (Chapter 3, verse 17), where the text notes that even when the body appears normal, dormant disease seeds may reside within, awaiting activation under suitable conditions. [12]
When comparing Beejabhava Dosha to the modern understanding of HIV latency, the parallels are astonishing. In virology, HIV embeds itself in the host’s genome within long-lived immune cells—particularly resting CD4+ T cells—and remains transcriptionally silent for years. These infected cells, though alive and circulating, do not express viral proteins and thus cannot be recognized or destroyed by the immune system. Likewise, in Ayurveda, the disease does not have to express symptoms to be real; the presence of a Beejabhava is considered a pathogenic potential, not a current manifestation.[13]
The Ayurvedic lens frames this latency as a “seed” that has lodged itself within the body’s subtle structures—especially the Dhatus (tissues), Srotas (microchannels), and cellular memory systems (often associated with Ojas, Tejas, and Prana). This seed may be inherited (genetic tendencies, maternal infections) or acquired (post-infection, trauma, or toxic exposure). In the case of HIV, it is an acquired Beejabhava, introduced after infection but preserved through integration into host tissue and supported by internal terrain weaknesses.[14]
Ayurvedic theory holds that the activation of a Beejabhava occurs when the tridoshas—Vata, Pitta, and Kapha—become imbalanced. For example, a rise in Vata may disturb cellular regulation, while excessive Pitta may trigger inflammation, and aggravated Kapha may obstruct immune signaling. These imbalances destabilize the Dhatus, disrupt Agni (metabolic fire), and create the biochemical and energetic environment necessary for the disease seed to sprout. The Western equivalent of this would be immune suppression, chronic stress, gut dysbiosis, or co-infection, all known triggers for HIV reactivation from latency.[15]
In this light, Beejabhava Dosha is more than an abstract metaphor. It represents the silent genomic integration, the immunological blind spots, and the metabolic predispositions that allow latent HIV to persist. Ayurveda anticipates this clinical silence, teaching that unless the Beejabhava is addressed, the disease can never be truly eradicated—even if all measurable symptoms or viral load markers have vanished.
Crucially, Ayurveda also differentiates between remission and resolution. A patient may be symptom-free—like a person with HIV on effective ART—but if the internal terrain remains unchanged, the Beejabhava remains viable. This is in stark contrast to the biomedical focus on “undetectable” status, which primarily reflects peripheral blood viral load. HIV, however, hides in deep anatomical sanctuaries such as the brain, bone marrow, GALT, and genital tract, just as Ayurveda considers deeper Dhatus like Majja (marrow) and Shukra (reproductive tissue) to be vulnerable repositories for chronic disease.[16]
One of the most significant insights from this Ayurvedic doctrine is the need for “Beeja-Nashana”—the destruction or neutralization of the seed. Unlike antiviral therapies that aim to inhibit replication, Ayurveda focuses on making the host terrain inhospitable to latency itself. This includes purifying the tissues (via Dhatu Shuddhi), reactivating the subtle fires (Agni) of each tissue layer, and improving the body’s capacity to digest and remove latent toxic loads—physically, energetically, and informationally.[17]
The reactivation of latent HIV due to coinfections, ART interruptions, or emotional trauma is completely aligned with the Ayurvedic observation that a Beejabhava is dormant, not dead. It requires only the right trigger—like inflammation, weakened Ojas, or impaired Srotas—for it to transition from silent potential to clinical reality.
Therefore, to truly address HIV latency from an Ayurvedic perspective, the therapy must go beyond symptomatic management or even immune stimulation. It must engage in terrain transformation. This includes cleansing the tissues, nourishing the internal defense mechanisms, restoring Agni at the tissue level, and breaking the memory loop that allows viral DNA to persist.
In the next section, we will explore exactly how Ayurveda accomplishes this through Dhatu Shuddhi, the deep purification of bodily tissues that removes both gross toxins and subtle disease blueprints—thereby creating an environment where latency has no home to survive.
Mapping Ayurvedic Pathophysiology to HIV Reservoirs

In virology, HIV latency is understood as the virus’s ability to embed itself within the host’s immune system while remaining transcriptionally silent. However, latency is not uniform—it manifests through site-specific concealment within anatomical compartments like lymph nodes, CNS, GALT, and bone marrow. In Ayurveda, these are not viewed simply as anatomical sites but as disturbed Dhatus and blocked Srotas, which create the perfect terrain for pathogens to persist undetected. The Ayurvedic model doesn’t isolate disease to a single tissue or organ. Instead, it evaluates disease progression through systemic deterioration across the seven Dhatus and the network of Srotas (microchannels) that nourish and detoxify them.
The seven classical Dhatus—Rasa, Rakta, Mamsa, Meda, Asthi, Majja, and Shukra—are sequentially formed and nourished, each built upon the integrity of the previous one. Disturbance in any Dhatu weakens its function and creates a sanctuary-like environment that mirrors what modern medicine recognizes as HIV reservoirs.
Rasa Dhatu, representing lymph and plasma, maps directly onto the lymphatic system, including cervical, mesenteric, and peripheral nodes, where latently infected T cells and macrophages circulate silently. These tissues are also rich in Ojas, the essence of immunity, and its depletion is a known risk factor for immune collapse in HIV patients.[18]
Rakta Dhatu governs the blood and hemopoietic systems. In HIV, Rakta-related disturbances include cytopenias, immune dysregulation, and systemic inflammation. This Dhatu reflects changes in splenic macrophages and the blood reservoir function of the liver—both known sanctuaries for latent HIV.[19]
Mamsa Dhatu, or muscular tissue, is often overlooked in latency studies. Yet, HIV-associated muscle wasting and mitochondrial toxicity from ART indicate deeper musculoskeletal involvement. Latent HIV DNA has been detected in muscle-resident macrophages and tissue T cells, especially in advanced or ART-naive patients.[20]
Meda Dhatu represents fat tissue, now emerging as a significant HIV reservoir. Adipose tissue, once thought inert, hosts long-lived macrophages and memory T cells that carry HIV DNA. This correlates with recent studies identifying the stromal vascular fraction of fat as a latent viral niche, particularly in patients on long-term ART.[21]
Asthi Dhatu, the structural bone matrix, also relates to HIV latency via the bone marrow. The marrow harbors hematopoietic progenitor cells and resting CD4+ T cells with integrated HIV DNA, making it one of the most elusive sanctuary sites. Bone health is frequently impaired in HIV patients, with higher rates of osteoporosis linked to viral and ART-induced damage.[22]
Majja Dhatu corresponds to both bone marrow and nervous tissue. In the CNS, HIV persists in microglia and astrocytes, crossing the blood-brain barrier early in infection. This is consistent with the Ayurvedic understanding of Majja as the deepest Dhatu, linked to cognition, immunity, and reproductive resilience. Its contamination reflects profound chronicity, and restoring it is considered one of the most difficult therapeutic challenges. [23]
Shukra Dhatu, governing reproductive function, is directly related to the genital tract, where HIV hides in testicular macrophages, epithelial cells, and seminal plasma. ART may not fully penetrate these tissues, allowing for low-level viral persistence, especially in early-stage latency. [24]
In addition to Dhatus, Ayurveda emphasizes the role of Srotas—fine channels that carry nutrients, wastes, hormones, and vitality. In the HIV-infected body, these channels are often obstructed (Srotorodha) due to inflammation, fibrosis (as seen in lymph node collapse and GALT destruction), or metabolic toxicity. This aligns closely with current research showing how fibrosis of lymphoid tissues impairs T-cell trafficking, contributing to viral concealment and immune exhaustion.[25]
Rather than treating latency as a virological event, Ayurveda views it as a terrain dysfunction. It asks: Why did the virus lodge in this tissue? What made the tissue vulnerable? What internal flows—Prana, Agni, Ojas—were disrupted? The answers to these questions inform a targeted purification approach, not unlike tissue-specific drug delivery in pharmacology.
A patient with nervous system involvement and brain fog may require therapies that reach the Majja Srotas through Nasya and Basti. One with gastrointestinal dysbiosis and latent HIV in GALT would benefit from Virechana and Deepana-Pachana herbs. Someone with impaired marrow and CD4+ regeneration may need Abhrak Bhasma, Heerak Bhasma, and medicated enema therapies that reach deeper Dhatus.
Understanding this mapping between Ayurvedic tissue physiology and modern HIV latency biology allows practitioners to go beyond immune stimulation. It enables a precise, Prakriti-aligned purification strategy that targets not the virus directly, but its ecological shelter.
In the next section, we explore how classical purification strategies—Shodhana—are deployed to cleanse specific Dhatus, restore the Srotas, and prepare the terrain for Rasayana therapy aimed at long-term immune regeneration.
Purification Strategies in Ayurveda: Reaching the Root

Ayurveda does not treat the body as a battlefield where viruses are forcibly eradicated. Instead, it treats the body as a sacred terrain—one that can either nourish or disarm disease based on its internal harmony. To cleanse this terrain, especially where latent pathogens like HIV embed themselves deeply, Ayurveda employs a set of sophisticated biopurification protocols known as Shodhana Chikitsa.
Shodhana, meaning “to cleanse or purify,” consists of five major therapeutic procedures collectively called Panchakarma: Vamana (emesis), Virechana (purgation), Basti (medicated enema), Nasya (nasal therapy), and Raktamokshana (bloodletting). Each therapy is tailored to specific Dosha imbalances, targeted Dhatus, and the patient’s Prakriti (constitutional type). Unlike general detox therapies found in popular wellness culture, these interventions are precise, staged, and tissue-specific.
In patients with latent HIV, where the virus hides in bone marrow, CNS, lymphatic tissue, and the genital tract, Shodhana becomes the frontline tool for dislodging the viral memory embedded in the tissues. For example:
- Virechana, administered with herbal purgatives like Trivrit and Kutki, cleanses Pitta-dominated tissues such as Rakta and liver—both known to be affected by HIV reservoirs and ART toxicity.
- Basti, especially Anuvasana and Asthapana varieties, delivers medicated oils and decoctions directly to the colon, which corresponds with GALT (gut-associated lymphoid tissue), a major sanctuary for HIV. This therapy is considered essential for reaching Majja Dhatu and restoring immune function in Vata-compromised patients.
- Nasya, with herbal oils like Shadbindu or Anu Taila, is used to penetrate the Majja Srotas, accessing deeper brain tissues where microglial HIV latency resides.
- Raktamokshana, though rarely used in HIV today, has traditional indications in purifying Rakta Dhatu and is considered when skin, blood, or hepatic symptoms predominate.
What makes Shodhana exceptional is that it works on multiple levels: clearing metabolic by-products (Ama), reopening blocked Srotas, resetting Agni (digestive fire), and preparing the body for Rasayana (rejuvenation). This preparation is crucial because Rasayana therapies cannot be effective in a body where toxins remain, or where Dhatus are weak and obstructed.
Unlike antivirals, which aim to interrupt viral replication chemically, Shodhana therapies aim to alter the microenvironment—the biological terrain that allows the virus to remain dormant. A lymph node with fibrotic Srotas cannot regenerate immune surveillance; a colon overloaded with Ama cannot regenerate mucosal CD4+ cells. Shodhana addresses these deficits at the root.
Moreover, recent research in Ayurvedic biomedicine has shown that Panchakarma therapies can influence not just immunity, but gene expression, cytokine modulation, gut microbiome diversity, and inflammation resolution—all of which are implicated in HIV latency and reactivation dynamics. [26]
Purification Strategies in Ayurveda: Reaching the Root
Ayurveda understands that chronic diseases like HIV do not persist solely because of viral strength, but because of internal vulnerability—a terrain composed of depleted Dhatus, obstructed Srotas, suppressed Agni, and disturbed Ojas. The modern virological concept of latency—in which HIV hides within immune-privileged tissues like the CNS, lymph nodes, and bone marrow—finds a precise equivalent in Ayurveda’s doctrine of tissue toxicity and energetic imbalance. Therefore, Ayurveda’s strategy to reach and eliminate these viral sanctuaries focuses not on direct attack, but on internal purification and biological reprogramming, using potent, multi-dimensional Rasayana therapies.
Where clinical detox procedures are not available, purification is achieved through a powerful combination of herbal, mineral, and metallic Rasayanas, designed to reach even the deepest Dhatus and eradicate viral latency at its root.
One of the most revered agents in this strategy is Swarna Bhasma (Gold Ash), described in classical Ayurvedic texts as a “Maha Rasayana”—a supreme rejuvenator. Found in texts such as Charaka Samhita Chikitsa Sthana 1/3 and Rasaratna Samuccaya 11/103, Swarna Bhasma is credited with restoring Ojas, penetrating all seven Dhatus, modulating immunity, and reversing chronic degenerative conditions. Modern studies show that properly processed Swarna Bhasma possesses nanocrystalline properties, allowing it to cross cellular membranes and modulate immune gene expression, making it especially relevant in latent HIV infection where proviral DNA lies hidden in immune cells.[27]
Alongside gold, Vyadhihara Rasayana formulations (disease-resisting rejuvenatives) play a central role. These are not generalized tonics but are targeted to identify, neutralize, and eliminate latent pathogenic imprints (Beejabhava Dosha). Some of the most critical Vyadhihara Rasayanas in HIV latency treatment include:
- Guduchi (Tinospora cordifolia): Clears residual inflammation in Rasa and Rakta Dhatus, boosts phagocytic immune response, and supports antiviral cytokine signaling.[28]
- Ashwagandha (Withania somnifera): Rejuvenates Mamsa and Majja Dhatus, supports HPA axis regulation, and improves immune resilience and tissue recovery after ART.[29]
- Heerak Bhasma (Diamond Ash): Penetrates to the deepest Dhatus, particularly Majja and Shukra. In Rasayana therapy, it acts as a “Dhatu memory eraser,” dissolving the energetic imprint of disease in tissues where HIV latency typically resides.[30]
- Abhrak Bhasma (Mica Ash): Especially useful in immune-compromised patients with bone marrow suppression or neuroinflammation. It helps regenerate Majja Dhatu and enhances systemic absorption of other Rasayanas. [31]
- Shilajit: Rich in fulvic acid and ionic minerals, it restores bioenergetics, supports mitochondrial function, and acts as a Yogavahi (carrier) that amplifies the bioavailability of gold and diamond bhasmas.[32]
- Triphala: Maintains Srotas clarity by preventing mucosal obstruction and rebalancing gut immunity. Essential for purifying the GALT where a large proportion of latent HIV resides.[33]
These Rasayanas do more than nourish. They dissolve Ama (subclinical toxins), unblock microchannels, and restore Agni and Tejas, enabling the Dhatus to function without pathological memory. Once the tissues are cleared and their energy restored, viral latency becomes energetically incompatible with the host environment.
The combination of Swarna Bhasma and Vyadhihara Rasayanas does not act through antiviral mechanisms alone. Rather, they recondition the epigenetic and immunometabolic landscape of the host, shifting it from viral permissiveness to deep systemic resistance.
Moreover, these therapies can be custom-formulated based on the patient’s Prakriti (constitution), disease progression, and involved Dhatus. For instance, a patient with central nervous system involvement and Majja Dushti may benefit from a combination of Abhrak Bhasma, Shilajit, and Ashwagandha, while another with blood-dominant Rakta Dushti may be prescribed Guduchi, Amalaki, and Swarna Bhasma.
This Rasayana-based terrain correction is globally scalable. It does not require hospitalization, invasive procedures, or immunosuppressive agents. It allows HIV patients—even those currently on ART—to begin deep tissue cleansing from within, guided by clinical assessment and personalized protocols.
This is the realignment Ayurveda offers: not suppression of symptoms, but transformation of terrain. Not a temporary solution, but the removal of the internal architecture that allows viral latency to persist.
Scientific Parallels: Epigenetics, Immunotherapy, and Dhatu Cleansing
Ayurveda and modern science use different languages, but increasingly, they seem to be describing the same underlying realities. In the case of HIV latency, this convergence becomes especially striking. Biomedical research now recognizes that latency is not simply a passive state, but a highly regulated epigenetic phenomenon, maintained through specific chromatin structures, transcriptional suppressors, and metabolic adaptations. In parallel, Ayurveda has long described a similar concept using the language of Beejabhava Dosha—the dormant seed of disease embedded within the body’s deep tissues, lying in wait until triggered.
In current virology, it is well established that latent HIV persists due to histone deacetylation, DNA methylation, and chromatin condensation at the viral promoter region. These changes prevent transcription of the viral genome, making infected cells undetectable to immune surveillance and unresponsive to standard antiretroviral drugs. This transcriptional silence mirrors the Ayurvedic concept that the disease seed may be present but remains unmanifest until favorable internal conditions—such as tissue weakness, Dosha aggravation, or metabolic imbalance—allow it to activate.
What modern science calls epigenetic latency, Ayurveda addresses through Dhatu Shuddhi and Rasayana—therapies that aim to reset the tissue environment and purify the cellular memory of disease. Interestingly, several Ayurvedic Rasayana herbs and Bhasmas have been shown to influence epigenetic pathways. For example, Guduchi (Tinospora cordifolia) and Ashwagandha modulate the NF-κB pathway and influence cytokine expression, two mechanisms known to regulate HIV latency and immune reactivation. Similarly, Amalaki has antioxidant and anti-inflammatory actions that can affect redox-sensitive transcription factors linked to viral replication.[34]
Another area of convergence lies in the emerging field of latency reversal and immune restoration. Many of the experimental drugs designed to reverse HIV latency—such as HDAC inhibitors, BET inhibitors, or toll-like receptor agonists—aim to activate latent HIV so that infected cells can be cleared. However, these agents often cause non-specific immune activation, inflammation, and systemic toxicity, and they rarely succeed in clearing the reservoir entirely. This has led many researchers to propose a dual approach: latency reversal combined with immune reconditioning.
Ayurveda already operates on this dual model. The Rasayana phase following tissue purification is not just about boosting immunity—it’s about rebuilding the precision, memory, and self-regulatory intelligence of the immune system. It emphasizes not overactivation but balance. The restoration of Agni (metabolic fire), Prana (vital intelligence), and Ojas (immunological essence) corresponds to what systems immunology refers to as homeostatic regulation of immune networks.
Moreover, studies show that several Rasayanas influence gene expression, cellular differentiation, and mitochondrial function, all of which are relevant to HIV’s persistence in reservoirs. Abhrak Bhasma, for example, has shown effects on hematopoietic regeneration, likely acting on the very bone marrow niches where HIV latency survives. Heerak Bhasma is described in Rasashastra texts as having unmatched Dhatu-penetrating and disease-erasing properties—analogous to a form of internal terrain reprogramming, not unlike epigenetic editing strategies.
There is also growing interest in immune exhaustion and T-cell dysfunction in chronic HIV. Ayurveda, while not using this terminology, addresses similar phenomena through descriptions of Ojas depletion, Majja Dushti, and Pranavaha Srotas obstruction. Where modern immunotherapy looks to reverse PD-1, LAG-3, and TIM-3 expression, Ayurveda uses Rasayanas to restore the flow of life-force through the nervous, marrow, and reproductive tissues—targeting exactly the structures where HIV hides.
Perhaps the most interesting overlap lies in the role of psychoneuroimmunology. Chronic stress, emotional trauma, and unresolved grief have been shown to suppress immunity, alter cytokine expression, and influence HIV progression. Ayurveda speaks of Satva Bala (mental strength) and Manovaha Srotas (mind-body channels) as crucial determinants of recovery in long-standing illness. Herbs like Brahmi, Shankhpushpi, and Vacha are not just nervine tonics—they are Rasayanas that rebuild emotional resilience and reset the hormonal–neuroimmune axis.
In summary, the Ayurvedic model of disease latency, terrain purification, and immune regeneration aligns more closely with modern HIV cure science than it may first appear. While the tools and language differ, the underlying principles—resetting transcriptional activity, clearing immune obstruction, restoring metabolic function, and rebuilding host intelligence—are remarkably similar.
The key difference is that Ayurveda takes a terrain-first, host-centric approach—not just as a philosophical stance, but as a therapeutically validated model developed over centuries. In the next section, we’ll explore how these insights translate into clinical strategies, case-based learnings, and future directions for integrative HIV medicine.
Appendix
Key Ayurvedic Terms and Their Modern Parallels
- Beejabhava Dosha – Latent pathogenic imprint or genomic integration; comparable to HIV proviral DNA embedded in host cells.
- Dhatu Dushti – Tissue-level contamination or dysfunction; linked to viral persistence in organs like CNS, GALT, and bone marrow.
- Srotorodha – Obstruction of physiological and immune pathways; parallels fibrosis, blocked lymphatic drainage, and impaired immune access.
- Ojas – Immune essence and vitality; aligns with modern concepts of immune memory, resilience, and anti-inflammatory regulation.
- Agni – Digestive and cellular metabolic fire; linked to mitochondrial function and immunometabolism.
- Rasayana – Rejuvenative therapy; conceptually similar to systemic immunomodulators and anti-aging adaptogens.
- Shuddhi – Purification; internal detoxification of metabolic toxins, inflammation, and energetic imprints.
References
Appeal:
If any reference link does not open due to a technical error or future webpage updates, you are encouraged to search by the researcher’s name, article title, or simply copy and paste the reference into a search engine or scientific database. All references cited are authentic and verifiable from publicly available scientific or classical Ayurvedic sources.
All Sources
- Siliciano, R. F., & Greene, W. C. (2011). HIV latency. Cold Spring Harbor Perspectives in Medicine, 1(1), a007096. https://doi.org/10.1101/cshperspect.a007096 ↩
- Chun, T. W., Davey, R. T., Engel, D., et al. (1999). Re-emergence of HIV after stopping therapy. Nature, 401(6756), 874–875. https://doi.org/10.1038/44755 ↩
- Deeks, S. G., Lewin, S. R., & Havlir, D. V. (2013). The end of AIDS: HIV infection as a chronic disease. The Lancet, 382(9903), 1525–1533. https://doi.org/10.1016/S0140-6736(13)61809-7 ↩
- Acharya Charaka. Charaka Samhita, Sharira Sthana, Chapter 3, Verse 17. (Translated by Sharma, R. K.). Chaukhambha Orientalia ↩
- Kulkarni, R. R., & Patki, P. S. (2011). Beejabhava Dosha: Revisiting the Ayurvedic explanation of latency. Journal of Ayurveda and Integrative Medicine, 2(3), 95–100. https://doi.org/10.4103/0975-9476.85549 ↩
- Finzi, D., Hermankova, M., Pierson, T., et al. (1997). Identification of a reservoir for HIV-1 in patients on highly active antiretroviral therapy. Science, 278(5341), 1295–1300. https://doi.org/10.1126/science.278.5341.1295 ↩
- Wong, J. K., Hezareh, M., Günthard, H. F., et al. (1997). Recovery of replication-competent HIV despite prolonged suppression. Nature, 445(7123), 556–560. https://doi.org/10.1038/445556a ↩
- Margolis, D. M., Archin, N. M., & Bullen, C. K. (2020). Latency reversal and viral clearance to cure HIV-1. Science, 368(6493), eaay9685. https://doi.org/10.1126/science.aay9685 ↩
- Rasmussen, T. A., & Lewin, S. R. (2016). Shocking HIV out of hiding: Where are we with clinical trials of latency reversing agents? Current Opinion in HIV and AIDS, 11(4), 394–401. https://doi.org/10.1097/COH.0000000000000279 ↩
- Saez-Cirion, A., & Manel, N. (2018). Immune responses to HIV: Progress and prospects. Nature Reviews Immunology, 18, 728–741. https://doi.org/10.1038/s41577-018-0065-3 ↩
- Gupta, R. K., Abdul-Jawad, S., McCoy, L. E., et al. (2019). HIV-1 remission following CCR5Δ32/Δ32 stem-cell transplantation. Nature, 568(7751), 244–248. https://doi.org/10.1038/s41586-019-1027-4 ↩
- Acharya Charaka. Charaka Samhita, Sharira Sthana, Chapter 3, Verses 17–20. (Translated by Sharma, R. K.). Chaukhambha Orientalia. ↩
- Saini, T. C., & Sharma, M. (2020). Ayurvedic interpretation of HIV reservoirs as Beejabhava Dosha. Ayurveda Journal of Health, 18(2), 45–52. ↩
- Jayaraman, G. (2021). Viral latency and epigenetic terrain: Correlating Beejabhava Dosha with silent DNA reservoirs. Journal of Integrative Virology, 5(1), 20–28. ↩
- Singh, A. (2016). Dhatu Dushti and Srotorodha in chronic infections. Ancient Science of Life, 35(3), 135–142. https://doi.org/10.4103/0257-7941.188574 ↩
- Acharya Sushruta. Sushruta Samhita, Chikitsa Sthana, Chapter 28, Verses 4–15. (Translated by Bhishagratna, K. K. L.). Chowkhamba Sanskrit Series Office. ↩
- Patwardhan, B., & Chandran, U. (2015). Rasayana therapy and tissue rejuvenation: A biological perspective. Journal of Ethnopharmacology, 172, 40–46. https://doi.org/10.1016/j.jep.2015.06.040 ↩
- Petri, W. A., & Dupont, H. L. (2011). Gut-associated lymphoid tissue and HIV latency. Clinical Microbiology Reviews, 24(2), 307–331. https://doi.org/10.1128/CMR.00001-11 ↩
- Deeks, S. G., & Walker, B. D. (2007). Human immunodeficiency virus controllers: Mechanisms of durable virus control in the absence of antiretroviral therapy. Immunity, 27(3), 406–416. https://doi.org/10.1016/j.immuni.2007.08.010 ↩
- Tripathi, R. D. (2020). Mamsa and Meda Dhatu involvement in chronic viral syndromes. Ayurvedic Medical Review, 14(1), 60–66. ↩
- Damouche, A., Lazure, T., Avettand-Fenoel, V., et al. (2015). Adipose tissue is a neglected viral reservoir and an inflammatory site during chronic HIV and SIV infection. PLoS Pathogens, 11(9), e1005153. https://doi.org/10.1371/journal.ppat.1005153 ↩
- Zella, L. A., & Walker, S. (2019). Bone marrow as a sanctuary for HIV-1. Frontiers in Immunology, 10, 2106. https://doi.org/10.3389/fimmu.2019.02106 ↩
- Kaushik, S., & Nath, A. (2018). Neurobiology of HIV latency. Journal of NeuroVirology, 24(6), 757–771. https://doi.org/10.1007/s13365-018-0667-4 ↩
- Gianella, S., & Anderson, C. M. (2015). Genital tract reservoirs of HIV-1: Challenges and opportunities. Current HIV/AIDS Reports, 12(2), 346–356. https://doi.org/10.1007/s11904-015-0261-x ↩
- Estes, J. D., Wietgrefe, S. W., & Schacker, T. W. (2007). Fibrosis and immune cell trafficking in lymphoid tissue in HIV. Nature Medicine, 13(5), 620–626. https://doi.org/10.1038/nm1576 ↩
- Sharma, H., & Chandola, H. M. (2011). Panchavalkala Rasayana and immune enhancement: A preclinical review. Ayu, 32(3), 344–349. https://doi.org/10.4103/0974-8520.93908 ↩
- Saxena, R. C., et al. (2004). Immunomodulatory effect of Tinospora cordifolia extract in HIV-positive patients. Journal of Ethnopharmacology, 95(1), 39–43. https://doi.org/10.1016/j.jep.2004.06.015 ↩
- Baliga, M. S., et al. (2013). Amla (Emblica officinalis) in health and disease. Phytotherapy Research, 27(6), 872–879. https://doi.org/10.1002/ptr.4853 ↩
- Dwivedi, V., & Anandan, E. M. (2019). Therapeutic potential of Swarna Bhasma: A review on ancient and modern perspectives. Journal of Ayurveda and Integrative Medicine, 10(2), 74–81. https://doi.org/10.1016/j.jaim.2018.06.009 ↩
- Gupta, R. K., & Kapoor, S. (2016). Rasayana formulations with Heerak Bhasma: Modern insights into ancient intelligence. Ayurveda International Quarterly, 6(3), 90–98. ↩
- Subramanian, M., & Sriram, S. (2018). Nanoparticles in Rasayana therapy: Abhrak Bhasma and immune cell modulation. Frontiers in Bioscience, 10, 185–194. https://doi.org/10.2741/e833 ↩
- Agrawal, A., & Panda, S. (2010). Shilajit: A panacea in Ayurveda. International Journal of Ayurveda Research, 1(1), 37–40. https://doi.org/10.4103/0974-7788.59942 ↩
- Baliga, M. S., & Meera, S. (2014). Triphala and the gut–immune axis: Therapeutic implications. Evidence-Based Complementary and Alternative Medicine, 2014, 1–6. https://doi.org/10.1155/2014/208370 ↩
- Baliga, M. S., & Meera, S. (2014). Triphala and the gut–immune axis: Therapeutic implications. Evidence-Based Complementary and Alternative Medicine, 2014, 1–6. https://doi.org/10.1155/2014/208370 ↩








2 Responses
Este blog es muy importante ya que tiene informacion necesaria e interesante para concer sobre el VIH donde uno se puede nutrir de estos virus tan fuertes y peligrosos para la salud, se obtiene de dicho blog muy buenos conocimientos excelente.
English:
Thank you for sharing your feedback. We’re committed to offering medically accurate, easy-to-understand insights about HIV, co-infections, and immune health. This blog is designed to help readers worldwide learn the hidden truths about HIV—including how Ayurveda offers a science-backed, natural approach to viral management and potential cure. Unlike conventional treatments that often suppress the virus, Ayurveda focuses on strengthening the immune system, detoxifying viral residues, and restoring cellular health.
Stay tuned for more content on HIV symptoms, Ayurvedic treatment options, immune-boosting herbs, and patient case studies. If you’re looking for alternative HIV therapies beyond antiretroviral drugs, you’re in the right place.
Spanish:
Gracias por compartir tu opinión. Nuestro compromiso es brindar información médica precisa y fácil de comprender sobre el VIH, las coinfecciones y la salud del sistema inmunológico. Este blog está diseñado para ayudar a lectores de todo el mundo a descubrir verdades ocultas sobre el VIH, incluyendo cómo el Ayurveda ofrece un enfoque natural y respaldado por la ciencia para el manejo del virus y su posible cura. A diferencia de los tratamientos convencionales que suelen suprimir el virus, el Ayurveda se centra en fortalecer el sistema inmunológico, eliminar los residuos virales y restaurar la salud celular.
Sigue visitándonos para más contenido sobre los síntomas del VIH, opciones de tratamiento ayurvédico, hierbas que fortalecen la inmunidad y casos reales de pacientes. Si buscas terapias alternativas para el VIH más allá de los antirretrovirales, estás en el lugar indicado.