

- Understanding Desmoid Tumor and GIST in Simple Clinical Terms
- Modern Medical Perspective
- Clinical Presentation
- The Most Common Global Mistake That Delays Proper Treatment
- Diagnostic Overlaps
- Step-by-Step Diagnostic Roadmap Every Patient Must Complete
- Common and Rare Disorders Associated With Desmoid Tumor and GIST
- High-Risk and Rare Complications That Can Become Life-Threatening
- Genetic and Syndromic Associations That Change the Entire Treatment Plan
- How Patients and Caregivers Increase Survival With a Proper Ayurvedic Integration Strategy
- Emergency Red-Flag Symptoms
- Treatment Challenges
- Treatment Pathways in the USA and UK – What Patients Must Know
- Living With Long-Term Therapy – Real Patient Challenges
- Financial Planning for Treatment – USA and UK Reality
- The Personal Medical File Every Patient Should Maintain
- Caregiver Guidance – What Families Must Monitor
- What “Cure” Really Means for Patients
- Ayurvedic Perspective
- Avaleha plus Rasayana-The Clinical Bridge for Root-Cause Reversal
- Ayurvedic Cure- Kanchnar Guggulu Avaleha(Medicine)
- Critical Warning – Do Not Use Market Avaleha or Self-Prepare Without Ayurvedic Medical Supervision
- Why Self-Preparation Is Equally Unsafe
- The Correct Clinical Model
- Comparative Cure Model – USA, UK and Ayurveda
- Hidden Truths & Critique
- Patient Decision Pathway – “Which Model Am I Currently In?”
- Integration Model – How a USA or UK Patient Safely Combines Oncology Care With Ayurveda
- Scan-to-Scan Survival Strategy – A Practical Framework for Patients and Caregivers
- Frequently Asked Questions (FAQ)
- References
Why This Guide Matters for Patients and Families
A diagnosis of a Desmoid tumor or a gastrointestinal stromal tumor (GIST) immediately places patients and their families into a rare disease pathway where correct decisions in the first few weeks can determine years of outcomes. These are not routine tumors. They require specialist pathology, mutation testing, long-term imaging strategies, and multidisciplinary planning. In both the USA and the UK, patients who enter sarcoma referral systems early have significantly better disease control, fewer unnecessary surgeries, and more personalized therapy plans. This guide exists to ensure that no patient loses time, receives incomplete diagnostics, or remains unaware of recurrence risk, long-term therapy implications, fertility considerations, financial planning, and systemic recovery strategies.
Desmoid tumor and GIST cure is achievable with a personalized integrative Ayurvedic treatment that works on tumor biology, metabolic correction, and long-term recurrence prevention instead of temporary disease control.
Desmoid tumors and GIST are rare stromal diseases that often require lifelong monitoring, complex treatment decisions, and specialist sarcoma care. This global patient and caregiver guide explains diagnosis, MDT pathways, recurrence risk, treatment options in the USA and UK, and how to build a long-term disease-control and recurrence-prevention strategy.
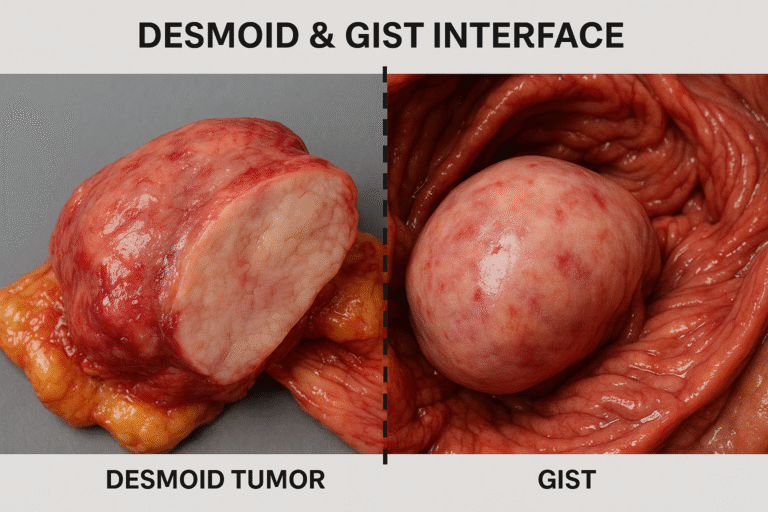
Most medical articles on Desmoid and GIST Tumors (GIST) present them separately, Desmoid as a “benign” fibromatosis and GIST as a “rare malignant stromal tumor.” What often gets overlooked is the shared interface between these conditions and the deeper lessons it offers in understanding tumor biology, recurrence, and healing. Our perspective is different: rather than isolating these tumors in silos, we explore their common ground, hidden truths, and the Ayurvedic lens that reframes them as part of a unified pathology.
Desmoid tumors and gastrointestinal stromal tumors are often described in modern oncology as conditions that can only be controlled.
However, long-term clinical experience shows that when tumor biology, systemic inflammation, metabolism, and tissue environment are corrected together, true disease reversal and sustained remission become possible in carefully selected patients.
Desmoid tumors are officially labeled as non-metastatic, yet in clinical practice they behave in ways that can be more devastating than some cancers [18]. Patients frequently undergo multiple surgeries, each followed by a high chance of recurrence, sometimes within months. They may cause bowel obstruction, organ dysfunction, or chronic pain severe enough to impair daily living [42]. Despite their benign label, many patients describe them as “benign but life-threatening,” a paradox rarely highlighted in standard oncology texts.
GIST tumors are better recognized for their malignant potential, driven by KIT and PDGFRA mutations. However, what is less often discussed is the fact that 10–15% of GISTs are “wild-type”—lacking these hallmark mutations—yet they still progress aggressively and resist standard targeted therapies [61]. Moreover, GIST is not confined to the stomach or small intestine; rarer cases arise in the rectum, esophagus, and even extra-gastrointestinal sites such as the omentum and mesentery [77]. These atypical presentations often lead to misdiagnosis or delayed treatment.
The interface between Desmoid and GIST lies in their overlapping challenges: both present as deep-seated abdominal masses, both can be mistaken for each other on imaging or histology, and both frustrate clinicians with long-term recurrence or drug resistance [84]. For patients, this often means a revolving door of hospital visits, experimental therapies, and anxiety about the future.
From an Ayurvedic perspective, this interface is even more meaningful. Ancient medical texts grouped such growths under Granthi (tumor-like swellings) and Arbuda (neoplastic growths), emphasizing their root in Dosha imbalance and Dhatu distortion. Where modern medicine sees separate rare diseases, Ayurveda sees a shared pathology of disturbed Agni (digestive-metabolic fire), vitiated Rakta and Mamsa Dhatus, and weakened Ojas (immunity-vitality) [109]. By bringing these two perspectives together, we not only expose the limitations of conventional management but also highlight how a root-cause-focused Ayurvedic approach can offer long-term solutions where modern therapies fall short [128].
This is what makes our exploration different: we do not simply describe tumors—we reveal their hidden interface, critique their under-recognized challenges, and provide a healing vision that bridges ancient wisdom with modern science.
Understanding Desmoid Tumor and GIST in Simple Clinical Terms
Desmoid tumors are biologically benign but clinically aggressive. They do not metastasize, yet they infiltrate surrounding structures, entangle bowel loops, compress nerves, and return even after apparently complete removal. Their behavior is unpredictable. Some remain stable for years, some regress spontaneously, and some enter repeated cycles of progression and intervention.
GIST is a molecularly driven stromal tumor. Its behavior is not defined by the word “cancer” but by its mutation, size, location, and mitotic activity. Many patients are cured with surgery alone. Others require years of targeted therapy. Some develop drug resistance and transition into a chronic disease model. Therefore, the real diagnosis is not “GIST,” but “GIST with a specific mutation and a specific risk category.”
Modern Medical Perspective

Pathophysiology
Understanding Desmoid Tumor and GIST in Simple Clinical Terms
Desmoid tumors and gastrointestinal stromal tumors (GISTs) differ significantly in their genetic and molecular drivers, but both share a mesenchymal origin.
Desmoid tumors arise primarily from mutations in the WNT/β-catenin signaling pathway, particularly CTNNB1 mutations. These mutations lead to excessive fibroblast proliferation and unchecked deposition of collagen, giving rise to the fibromatosis phenotype [34]. Though benign in classification, their aggressive local infiltration mimics the behavior of malignant tumors. What is lesser known is that familial adenomatous polyposis (FAP) patients have a markedly higher risk of desmoid tumors due to APC gene mutations, linking desmoid growth with colon cancer syndromes [52].
GIST tumors are driven in most cases by gain-of-function mutations in KIT or PDGFRA, leading to continuous tyrosine kinase signaling and abnormal cell proliferation [63]. However, a subset—referred to as wild-type GISTs—lack these common mutations yet display aggressive clinical behavior. Many of these are associated with defects in the succinate dehydrogenase (SDH) complex, connecting tumor biology to mitochondrial dysfunction [79]. This aspect is rarely discussed in general reviews but highlights why certain GISTs resist standard tyrosine kinase inhibitors (TKIs).
At the interface, both desmoid and GIST tumors underscore a key problem in oncology: stromal tumors that defy neat classification as benign or malignant, challenge therapeutic predictability, and highlight the inadequacy of one-size-fits-all strategies [91].
Clinical Presentation

Desmoid tumors most frequently arise in the abdominal wall, intra-abdominal region, and extremities, though they can develop in virtually any connective tissue site [24]. They are considered non-metastatic, yet their locally aggressive nature often leads to complications that mimic or even surpass those of malignant tumors. Patients may present with firm, deep-seated masses, progressive pain, restricted mobility, or even bowel obstruction when tumors infiltrate the mesentery [47]. A lesser-known fact is that pregnancy can accelerate the growth of desmoid tumors, likely due to hormonal influences on fibroblast proliferation [66].
Gastrointestinal stromal tumors (GISTs) predominantly occur in the stomach (60%) and small intestine (30%), but rare cases are also seen in the colon, rectum, esophagus, and extra-gastrointestinal locations such as the omentum and mesentery [72]. Clinical manifestations often include vague abdominal pain, gastrointestinal bleeding, anemia, or palpable mass. In advanced cases, metastasis most commonly targets the liver and peritoneum [88]. Importantly, small GISTs (<2 cm) may remain clinically silent and are sometimes discovered incidentally during imaging or surgery for unrelated conditions [97].At the interface, both Desmoid and GIST tumors can present with abdominal masses, obstruction, or pain, creating diagnostic overlap and sometimes misclassification on initial imaging [115]. While Desmoids rarely spread, their relentless local infiltration may lead to repeated surgical interventions. GISTs, in contrast, may metastasize but occasionally remain indolent for years. This paradox highlights the difficulty clinicians face: a benign tumor that behaves malignantly, and a malignant tumor that can masquerade as benign.
The Most Common Global Mistake That Delays Proper Treatment
The biggest preventable error worldwide is management outside a sarcoma multidisciplinary system. When biopsy, surgery, or drug therapy begins before expert pathology and molecular classification, patients often undergo:
- incomplete resections
- avoidable recurrence
- incorrect drug selection
- delayed targeted therapy
In both the USA and the UK, early referral to a sarcoma center changes the entire disease trajectory.
Diagnostic Overlaps

Imaging similarities remain a central challenge in differentiating Desmoid tumors from GIST. On CT and MRI scans, both may present as well-defined or infiltrative soft tissue masses in the abdomen [36]. Desmoid tumors often appear as iso- to hypointense masses on T1-weighted MRI and heterogeneously hyperintense on T2, while GISTs can mimic this spectrum, particularly when located in the mesentery or retroperitoneum [59]. Even PET scans do not reliably separate them, as both lesions may show increased FDG uptake, leading to misinterpretation [83]. This overlap is one reason patients are sometimes misdiagnosed and subjected to inappropriate therapies.
Histology adds another layer of complexity. Both Desmoid and GIST tumors may display a spindle-cell morphology, a pattern seen in many soft tissue tumors [92]. While Desmoid tumors characteristically demonstrate long sweeping fascicles of fibroblasts within a collagen-rich stroma, and GISTs exhibit spindle or epithelioid cells, the microscopic overlap can be misleading in small biopsy samples [108]. Therefore, immunohistochemistry (IHC) is essential for distinction:
- Desmoid tumors show nuclear β-catenin positivity due to WNT pathway activation.
- GISTs demonstrate strong positivity for c-KIT (CD117), DOG1, and often CD34, reflecting tyrosine kinase activation [124].
Differential diagnostic challenges are amplified in cases of extra-gastrointestinal GIST (EGIST) and intra-abdominal desmoid tumors, which both occur in the mesentery. Such cases can appear indistinguishable on imaging and histology until molecular testing is performed [139]. Misclassification is not just academic—patients with desmoid tumors may be unnecessarily placed on tyrosine kinase inhibitors (TKIs), while GIST patients may undergo incomplete resection due to mistaken benign labeling. These pitfalls demonstrate the urgent need for integrated diagnostic algorithms that combine imaging, histology, IHC, and molecular profiling [151].
From an Ayurvedic lens, both conditions fall under Arbuda and Granthi categories where external imaging cannot reveal the deeper Dosha–Dhatu imbalance. Instead, Ayurveda emphasizes Nidana Panchaka—the fivefold diagnostic approach assessing causation, premonitory signs, specific features, pathogenesis, and systemic involvement. This philosophical difference highlights why modern scans may confuse, while Ayurveda seeks to understand the internal terrain that allows such growths to persist.
Step-by-Step Diagnostic Roadmap Every Patient Must Complete
Every patient must complete three pillars of diagnosis.
First, correct imaging. Desmoid tumors are best followed with contrast MRI to assess soft-tissue infiltration. GIST requires contrast CT to evaluate primary site and metastatic spread. The first scan becomes the lifetime comparison baseline.
Second, expert pathology. The pathology report must clearly state the immunohistochemistry profile. In desmoid, nuclear beta-catenin confirms the diagnosis. In GIST, c-KIT and DOG1 establish stromal origin.
Third, molecular testing for GIST. This is not optional. The mutation determines whether imatinib will work, whether alternative drugs are needed, and how long treatment continues. Without this information, therapy is incomplete.
Common and Rare Disorders Associated With Desmoid Tumor and GIST

A Life-Saving Guide for Patients and Caregivers
These tumors affect far more than the visible mass. Many life-threatening situations arise from bleeding, obstruction, organ compression, treatment toxicity, genetic syndromes, or delayed recognition of progression. Patients and caregivers who understand these patterns act earlier, reach the correct specialist sooner, and avoid emergency deterioration. This section explains what to watch, why it happens, and how a properly supervised Ayurvedic support strategy fits safely during the stable phases of care.
Gastrointestinal Bleeding and Chronic Anemia
Why this happens
GIST frequently develops in the stomach or small intestine where the tumor surface becomes fragile and ulcerates. This causes slow internal bleeding or sudden hemorrhage. Many patients are treated for “low hemoglobin” for months before the tumor is detected.
What patients and caregivers must watch
Black stools, vomiting blood, new paleness, breathlessness on mild activity, dizziness, rapid heartbeat, or sudden exhaustion are danger signals. Even mild long-term fatigue with falling hemoglobin requires urgent evaluation.
Why early action saves life
Untreated bleeding leads to severe anemia, cardiac strain, and collapse. Early endoscopy or imaging prevents emergency surgery.
Where Ayurveda supports safely
During stable disease, physician-guided therapy focuses on improving digestion, appetite, strength, and Rakta support so the patient tolerates oncology treatment and recovers faster. It never replaces emergency care for active bleeding.
Abdominal Mass Effect, Pain, Early Satiety and Malnutrition
Why this happens
Desmoid tumors infiltrate tissues and GIST grows within the gastrointestinal tract. Both create pressure on surrounding organs. Patients feel full after a few bites, lose weight, and gradually become weak.
What patients and caregivers must watch
Reduced food intake, visible abdominal distension, increasing pain after meals, progressive weight loss, or inability to finish normal portions.
Why early action saves life
Malnutrition reduces immunity, delays wound healing, increases drug toxicity, and weakens survival.
Where Ayurveda supports safely
A properly designed Avaleha under supervision helps restore appetite, improve bowel rhythm, and rebuild strength during the non-emergency phase. The formulation must match Agni and disease stage.
Intestinal Obstruction and Sub-Obstruction
Why this happens
Intra-abdominal desmoid tumors compress bowel loops. GIST can narrow the intestinal lumen. Initially this causes intermittent symptoms and later complete obstruction.
What patients and caregivers must watch
Repeated bloating, severe constipation, vomiting after meals, crampy abdominal pain, inability to pass gas, or sudden abdominal distension.
Why early action saves life
Partial obstruction detected early can be managed in a planned manner. Late detection leads to emergency surgery, perforation, infection, and intensive care admission.
Where Ayurveda supports safely
In the stable phase, therapy focuses on maintaining digestive rhythm and reducing Ama so bowel function remains regular. No internal medicine should be taken during suspected obstruction without medical clearance.
Long-Term Targeted Therapy–Related Systemic Disorders
Why this happens
Tyrosine kinase inhibitors control disease for years but create chronic metabolic load.
What patients and caregivers must watch
Persistent fatigue, swelling around eyes or legs, chronic diarrhea, loss of appetite, muscle wasting, sleep disturbance, skin changes, and reduced daily activity.
Why early action saves life
These symptoms lead to silent dose skipping. Irregular drug intake allows tumor regrowth and resistance.
Where Ayurveda supports safely
Supervised integrative care improves digestion, sleep quality, muscle strength, and daily stamina so treatment continues without interruption. Liver and blood parameters must be monitored alongside oncology care.
High-Risk and Rare Complications That Can Become Life-Threatening
Ureteric Compression and Kidney Damage
Why this happens
Pelvic or mesenteric desmoid tumors compress the ureters and block urine flow.
What patients and caregivers must watch
Flank pain, recurrent urinary infection, reduced urine output, swelling of legs, or rising creatinine in reports.
Why early action saves life
Untreated hydronephrosis leads to permanent kidney damage and sepsis.
Where Ayurveda supports safely
After decompression and stabilization, Rasayana-based tissue support helps recovery of strength and metabolic balance.
Bowel Ischemia, Perforation, Fistula and Intra-Abdominal Abscess
Why this happens
Deep infiltrative desmoid disease compromises blood supply or erodes into adjacent bowel.
What patients and caregivers must watch
Sudden severe abdominal pain, fever, rigid abdomen, vomiting, or signs of infection.
Why early action saves life
This is a surgical emergency. Delay can lead to septic shock.
Where Ayurveda supports safely
Only in the recovery phase after emergency management, to rebuild Dhatu and improve long-term resilience.
Tumor Rupture and Acute Abdomen in GIST
Why this happens
Large or rapidly growing tumors can rupture, causing internal bleeding and peritonitis.
What patients and caregivers must watch
Sudden collapse, severe pain, black stools with weakness, fainting, or low blood pressure.
Why early action saves life
Immediate hospitalization is required. Time lost at home can be fatal.
Where Ayurveda supports safely
Post-stabilization recovery and long-term recurrence prevention.
Genetic and Syndromic Associations That Change the Entire Treatment Plan
Familial Adenomatous Polyposis and Gardner Syndrome
Why this matters
Desmoid tumors are a major cause of illness and death in FAP. These patients require lifelong surveillance and family screening.
What families must do
If there is a history of multiple colon polyps or early colon cancer, genetic evaluation is essential. Relatives may also be at risk.
Integrative relevance
Long-term terrain correction becomes a parallel preventive strategy after oncology stabilization.
Neurofibromatosis Type 1 Associated GIST
Why this matters
These tumors follow a different biological pattern and require a modified surveillance plan.
What patients must disclose
Skin nodules, café-au-lait spots, or known NF1 diagnosis.
SDH-Deficient GIST, Carney Triad and Carney-Stratakis Syndrome
Why this matters
These conditions involve tumors outside the gastrointestinal tract such as paraganglioma or lung lesions.
What patients and caregivers must watch
Unexplained hypertension episodes, palpitations with headache, neck masses, or lung nodules.
Life-saving step
Surveillance must include other organs, not only the abdomen.
How Patients and Caregivers Increase Survival With a Proper Ayurvedic Integration Strategy
Early Danger Recognition and Immediate Oncology Escalation
Ayurveda is never used in place of emergency care. Its life-saving role is early detection of imbalance and strengthening the patient between scans so complications are reported before they become critical.
Terrain Correction During the Stable Phase
When scans show control or after recovery from surgery, the internal environment becomes the focus. Agni correction, Ama reduction, Dhatu rebuilding and Ojas restoration improve long-term stability and reduce recurrence tendency. This phase is where a physician-designed Avaleha plus Rasayana protocol is most valuable.
Maintaining Treatment Continuity and Strength
The greatest survival advantage in modern stromal tumor care is uninterrupted therapy. When patients have stable digestion, good sleep, strong muscles, and mental resilience, they continue treatment regularly and outcomes improve.
Emergency Red-Flag Symptoms
Every Caregiver Must Treat as Immediate Hospital Situations
Severe or rapidly increasing abdominal pain, persistent vomiting, inability to pass stool or gas, black stools or vomiting blood, fainting, high fever with abdominal pain, sudden weakness with low blood pressure, or new flank pain with urinary symptoms.
Recognizing these early and acting without delay is one of the most powerful ways families save lives in Desmoid and GIST care.
Treatment Challenges

Desmoid tumors remain one of the most paradoxical conditions in oncology. Although non-metastatic, their unpredictable growth and relentless local infiltration make them extremely difficult to manage. Historically, surgery was the frontline therapy, but recurrence rates of up to 70% after resection have forced clinicians to reconsider [27]. Today, management often involves a combination of NSAIDs, anti-estrogen therapy (tamoxifen, toremifene), and tyrosine kinase inhibitors (TKIs) such as sorafenib or pazopanib [48]. Radiotherapy has been used in selected cases, but its long-term safety in young patients is questionable [65]. A crucial yet lesser-discussed fact is the role of a “watch-and-wait” strategy, where some desmoid tumors spontaneously stabilize or regress without active intervention [81]. This has shifted guidelines toward a more conservative approach, but it leaves patients in prolonged uncertainty.
Gastrointestinal stromal tumors (GISTs) revolutionized the field of targeted cancer therapy with the advent of imatinib, a TKI that directly inhibits KIT and PDGFRA signaling [94]. For patients resistant to imatinib, second-line (sunitinib) and third-line (regorafenib) therapies exist, but each carries the looming problem of acquired resistance over time [116]. Surgical resection remains important for localized tumors, but unlike desmoids, GIST surgery alone is rarely curative without systemic therapy. Furthermore, chemotherapy and radiation offer almost no benefit, making TKIs the cornerstone of therapy [133]. A hidden challenge is that wild-type and SDH-deficient GISTs often respond poorly to imatinib, leaving patients with limited alternatives [147].
At the interface, both Desmoid and GIST tumors expose a shared set of challenges:
- Long-term therapy dependency: Patients often require chronic medication or multiple surgeries.
- Drug resistance: Desmoids show variable response to TKIs, while GISTs frequently develop secondary resistance mutations.
- High recurrence burden: Desmoids recur locally despite aggressive management, and GISTs recur systemically despite targeted therapy [162].
From an Ayurvedic perspective, these challenges are seen as the ineffectiveness of symptomatic management without addressing the root imbalance. Ayurveda emphasizes therapies that restore Agni (digestive-metabolic balance), cleanse Doshas through Shodhana, and rebuild Ojas (vital immunity) with Rasayana formulations, aiming to prevent recurrence rather than perpetuate lifelong treatment cycles [179].
Treatment Pathways in the USA and UK – What Patients Must Know
For desmoid tumors, modern global practice increasingly begins with active surveillance. This is not neglect. It is a biologically informed decision, because many tumors stabilize or regress. Treatment is initiated only when there is pain, organ risk, functional impairment, or clear progression on serial imaging.
When treatment is required, the goal must be defined clearly. Some therapies aim for shrinkage. Others aim for stability. Surgery is now reserved for carefully selected cases because repeated operations increase morbidity.
For GIST, treatment is risk-adapted. Localized low-risk tumors may need surgery alone. Intermediate and high-risk tumors require adjuvant targeted therapy for defined durations. Metastatic disease becomes a long-term targeted therapy pathway with sequential drugs.
The most important patient question is not “What is the treatment?” but “What is the objective of this treatment in my risk category?”
Living With Long-Term Therapy – Real Patient Challenges
Long-term targeted therapy affects:
- energy levels
- fluid balance
- digestion
- skin
- muscle strength
- hormonal health
- fertility planning
- pregnancy timing
These are not minor side effects. They define quality of life and adherence to treatment. A successful plan includes proactive management of these effects, not reactive symptom control.
Financial Planning for Treatment – USA and UK Reality

Financial planning in Desmoid and GIST care is not a background administrative task. It directly determines whether treatment starts on time, whether it continues without interruption, and whether surveillance imaging happens at the correct interval. In long-duration diseases where therapy may extend for years, financial instability becomes a biological risk factor. When patients delay scans, reduce doses, or interrupt targeted therapy because of cost or access barriers, the disease does not pause. This is why financial preparation must begin at the same time as medical planning.
United States- Advanced Treatment With Access Filtered by Insurance Structure
In the United States, the most sophisticated therapies are available, but access is governed by insurance approval pathways. Genomic testing, specialist sarcoma consultations, oral targeted therapy, and repeated contrast imaging often require prior authorization. Many patients discover that the recommended treatment and the immediately accessible treatment are not always the same.
High out-of-pocket costs for oral anticancer drugs are strongly associated with reduced adherence and early discontinuation. Patients may quietly delay starting therapy, split doses to make medication last longer, or postpone scans because of co-payments. These decisions are rarely discussed during consultations, yet they have measurable clinical consequences in long-term disease control. Financial strain is also linked to employment instability, and loss of employment can lead to loss of insurance, creating a cycle that affects both medical continuity and mental health.
Early involvement of a financial counselor or patient navigator allows patients to clarify coverage for mutation testing, understand co-pay responsibilities for long-term therapy, access manufacturer assistance programs, and plan imaging approvals based on risk category. This proactive approach prevents forced treatment interruption later in the disease course.
United Kingdom-Universal Coverage With Time and Pathway Constraints
In the United Kingdom, core treatment is delivered through the NHS sarcoma referral network, which removes the direct drug-cost burden from patients. However, financial toxicity appears in a different form. The hidden pressures are related to time, travel, and system capacity.
Patients must understand which sarcoma center is responsible for their care, the exact interval between surveillance scans, and the criteria that trigger treatment escalation. When imaging intervals are extended beyond what the individual tumor biology requires, progression may occur before the next review. Travel to regional specialist centers, time away from work for repeated appointments, and delays in accessing second opinions create a cumulative financial and emotional burden for families.
For patients who do not respond to standard therapy, early discussion of clinical trial referral is essential, because access is often centralized and time-sensitive.
The Psychological Cost of Financial Toxicity
Financial stress is consistently associated with higher symptom burden, reduced treatment adherence, poorer quality of life, and worse survival outcomes in oncology populations. In Desmoid and GIST, where the treatment journey often spans many years, this stress becomes chronic. Patients are frequently told that therapy will continue long term, but they are not guided through how this interacts with employment, fertility planning, travel, or medication access during life transitions. This gap between medical prescription and real-life logistics is one of the most common causes of silent non-adherence.
Drug Dependency Without a Long-Term Life Plan
Targeted therapy is often presented as convenient because it is oral, yet the long-term reality includes fatigue, fluid retention, gastrointestinal disturbance, frequent monitoring, and ongoing prescription logistics. Patients and families must plan for how medication will be maintained during job changes, relocation, pregnancy planning, or extended travel. Without this planning, treatment interruptions occur at the most biologically vulnerable moments.
The Caregiver as the Financial and Logistical Coordinator
Caregivers frequently become responsible for insurance communication, reimbursement claims, appointment scheduling, medication supply continuity, and transport to specialist centers. This role is rarely acknowledged in the treatment plan, yet caregiver stability directly affects whether therapy continues on schedule. Caregiver burnout is strongly associated with financial strain and can indirectly worsen patient outcomes.
Why Financial Stability Is a Medical Priority
In GIST, interruption of tyrosine kinase inhibitor therapy can allow tumor progression and promote resistant cellular clones. In Desmoid disease, delayed imaging can shift management from planned medical therapy to emergency intervention with higher morbidity. Financial stability therefore determines continuity of therapy, timing of surveillance, access to specialist care, psychological resilience, and long-term disease control. In rare stromal tumors, a secure financial pathway is not a social advantage; it is a core component of medical strategy.
The Personal Medical File Every Patient Should Maintain

In rare tumors such as Desmoid and GIST, the most empowered patients are those who maintain their own complete medical record. Hospitals change, doctors rotate, insurance networks shift, and second opinions may happen in different cities or even different countries. A structured personal medical file ensures continuity of care, prevents loss of critical information, and allows faster and more accurate clinical decisions. It converts the patient from a passive recipient of fragmented updates into an informed participant in long-term disease strategy.
Why This File Is Clinically Important
These diseases are followed for years, sometimes for life. Treatment decisions are not made from memory, they are made by comparing timelines. Tumor behavior is judged by millimeter changes across serial scans. Drug tolerance is understood only when side effects are mapped against dose adjustments. Risk of recurrence is assessed from original pathology, not from the latest prescription. When this information is scattered across multiple institutions, delays and errors become common. A well-maintained personal file allows any sarcoma specialist or multidisciplinary team to understand the entire journey within minutes.
Core Diagnostic Documents
The first section of the file should contain all primary diagnostic material. This includes the initial radiology reports and the images themselves in digital format, not just the written summary. Pathology must be preserved in its complete form, including immunohistochemistry and, for GIST, the full mutation analysis. The original tumor size, mitotic rate, anatomical location, and margin status are not historical details. They define present and future treatment decisions.
Treatment Timeline
A clearly written chronological treatment history is essential. Each therapy should be listed with its exact start date, any dose modification, temporary interruption, and stop date. For targeted therapies, the reason for each dose change must be recorded, whether it was toxicity, planned reduction, progression, or financial interruption. This allows a new clinician to understand what has truly been tried and what remains a valid option.
Scan Tracking and Tumor Measurement Log
Patients should maintain a simple but precise record of every scan date with the key tumor measurements. This is more valuable than storing reports alone. When tumor size is plotted over time, patterns become visible: stability, slow progression, treatment response, or regrowth after interruption. These patterns are the basis of real clinical decisions. Without them, management becomes reactive rather than planned.
Side-Effect and Quality-of-Life Mapping
Long-term therapy is not defined only by tumor response. Fatigue, edema, gastrointestinal disturbance, muscle loss, hormonal changes, sleep disruption, and mood alterations determine whether treatment is sustainable. Recording when a side effect started, how severe it became, and whether it improved after dose adjustment allows doctors to balance disease control with quality of life. This also prevents unnecessary discontinuation of a drug that might be effective if toxicity is managed early.
Administrative and Access Documents
A complete file should also include insurance approvals, drug authorization letters, clinical trial eligibility assessments, and contact details of the treating sarcoma center. In the UK, this means documenting the responsible MDT and follow-up schedule. In the USA, this means tracking authorization validity for scans and medication. These administrative elements often determine how quickly care can continue.
Format and Practical Use
The file can be maintained in both digital and printed form. Digital storage should include scan images on secure cloud access so they can be shared instantly for second opinions. A concise printed summary should travel with the patient for consultations. The goal is not to store documents, but to create a readable disease timeline that any specialist can interpret quickly.
How This Changes Outcomes
When patients bring a complete medical file to a consultation, the discussion moves immediately to strategy rather than reconstruction of history. Second opinions become precise and meaningful. Emergency decisions are avoided because progression is detected earlier. Treatment is not repeated unnecessarily. Most importantly, the patient regains a sense of control in a disease that otherwise feels unpredictable.
Maintaining this file is not a clerical task. It is a clinical tool and one of the most powerful forms of self-advocacy available to patients and caregivers navigating long-term Desmoid or GIST care.
Caregiver Guidance – What Families Must Monitor

In long-duration conditions such as Desmoid tumor and GIST, caregivers are not only providing emotional support. They are often the first people to notice subtle biological changes that occur between scheduled scans and clinic visits. Tumor behavior does not always declare itself through dramatic symptoms. It frequently begins with small functional changes, altered daily patterns, or new forms of discomfort that the patient may normalize or underreport. Early recognition of these changes allows timely medical review and prevents emergency interventions.
Why the Caregiver’s Observation Is Clinically Valuable
Most follow-up in these diseases is interval-based. Imaging may be scheduled every three to six months, and consultations may be brief. During this time, the person who sees the patient every day becomes the most reliable continuous observer of disease behavior. Patients often minimize symptoms to avoid worry, to continue working, or because they have adapted to chronic discomfort. Caregivers, however, notice deviation from the patient’s normal baseline. This makes their input medically important, not merely supportive.
New or Changing Pattern of Pain
Pain related to stromal tumors is usually not constant. A change in its pattern is more significant than its intensity. Pain that begins to occur at a different time of day, appears during previously comfortable activities, radiates to a new location, or starts disturbing sleep can indicate structural progression or pressure on adjacent tissues. Reporting this early allows imaging to be advanced before functional loss occurs.
Change in Bowel or Digestive Function
For intra-abdominal Desmoid disease and GIST, bowel function is a sensitive clinical indicator. Increasing bloating, early satiety, new constipation, altered stool caliber, intermittent obstruction-like symptoms, or unexplained nausea may reflect evolving mass effect long before it becomes visible externally. These symptoms should not be attributed automatically to diet, stress, or medication without medical review.
Unexplained Fatigue or Decline in Daily Stamina
Targeted therapies and chronic tumor activity both influence metabolic energy. A noticeable drop in the patient’s usual stamina, longer recovery time after routine tasks, or increased daytime sleep may indicate anemia, drug toxicity, nutritional compromise, or disease progression. Because fatigue develops gradually, patients often do not perceive its magnitude. Caregivers comparing current function with the patient’s previous baseline can identify this change earlier.
Reduced Mobility or Postural Change
Slower walking speed, difficulty rising from a chair, protective body posture, reduced arm swing, or avoidance of certain movements may signal pain, nerve involvement, muscle loss from therapy, or increasing intra-abdominal pressure. These physical adaptations often appear weeks before patients report “difficulty moving.”
Emotional Withdrawal or Behavioral Change
Psychological changes are not separate from the disease process. Sudden quietness, reduced engagement in conversation, withdrawal from social interaction, loss of interest in previously meaningful activities, or increased irritability may reflect uncontrolled symptoms, drug intolerance, fear of progression, or financial stress. These changes affect adherence to therapy and willingness to attend follow-up appointments. Early acknowledgement allows supportive intervention before isolation develops.
Treatment Tolerance and Medication Continuity
Caregivers are often the first to recognize missed doses, reluctance to take medication, new swelling, persistent diarrhea, skin changes, or altered appetite. Long-term oral therapy only works when taken consistently. Detecting intolerance early allows dose adjustment rather than silent discontinuation.
The Importance of Timely Communication
Reporting these changes does not mean demanding immediate intervention. It means informing the treating team early enough to decide whether imaging should be advanced, laboratory tests repeated, dose modified, or supportive care introduced. This transforms care from crisis-based to strategy-based.
The Caregiver as a Clinical Partner
Families should be encouraged to maintain a simple parallel observation record noting the date when a new symptom or functional change first appeared. This provides objective information during consultations and prevents loss of detail. When caregivers are recognized as part of the clinical ecosystem, outcomes improve because monitoring becomes continuous rather than episodic.
Early observation, early communication, and early adjustment of the treatment plan prevent emergency hospitalizations, preserve organ function, maintain quality of life, and reduce psychological distress for both patient and family.
What “Cure” Really Means for Patients

In Desmoid tumor and GIST care, the word cure carries different meanings depending on who is using it. For patients and families, cure is not a statistical endpoint. It is a lived reality. It means the disappearance of disease from daily life, freedom from continuous therapy, and the ability to plan the future without the shadow of the next scan. For oncology systems, success is often defined as long-term disease control or stable imaging. Ayurveda introduces a third and fundamentally different framework, where cure is defined as complete resolution of the pathological process through restoration of Dosha, Agni, Dhatu, Mala, and Ojas equilibrium.
The Ayurvedic Definition of Cure – Root-Level Reversal of Samprapti
Ayurveda does not define health merely as absence of a visible mass. The classical definition of health clearly states that true recovery occurs only when systemic balance is restored:
“Samadoshah samagnischa samadhatu malakriyah
Prasanna atmendriya manah swastha ityabhidhiyate.”
— Sushruta Samhita, Sutra Sthana 15/41
Meaning: A person is healthy only when Dosha are balanced, Agni is normal, Dhatu and Mala function properly, and the mind and senses are in a state of wellbeing.
From this perspective, a tumor is not an isolated structural defect. It is the final manifestation of a long-standing internal imbalance. Therefore, true cure requires reversal of the entire pathological cascade, not only removal or suppression of the mass.
Arbuda and Granthi – Classical Correlation With Stromal Tumors
Desmoid and GIST share features with the Ayurvedic descriptions of Granthi and Arbuda, where localized growth develops due to deep-seated Dosha–Dhatu vitiation.
“Mamsa shonita medobhih granthir mandalavritah
Shopho alpavedano dirghakala anubandhi cha.”
— Sushruta Samhita, Nidana Sthana 11/13
This describes a firm, slowly progressive, deep-seated growth arising from vitiated Mamsa, Rakta, and Meda Dhatu, with chronicity and structural infiltration, closely resembling the biological behavior of stromal tumors.
For Arbuda, the classical texts emphasize its origin from profound Dosha accumulation and Dhatu dushti:
“Dosha medomamsa asruk sannipatah sthiram mahat
Mandaruja anubandham cha arbudam iti lakshanam.”
— Sushruta Samhita, Nidana Sthana 11/3
The pathology is not only local. It is systemic, involving metabolic failure, tissue-level dysfunction, and impaired immune intelligence.
Why Suppression Alone Is Not Considered Cure in Ayurveda
Ayurveda clearly differentiates between temporary palliation and complete eradication of disease process.
“Yat punar na bhavet vyadhi tat chikitsitam uttamam.”
— Charaka Samhita, Chikitsa Sthana 1/4
Meaning: That treatment is superior after which the disease does not recur.
This principle directly addresses the modern challenge of lifelong drug dependency and recurrence. If the internal terrain remains unchanged, the disease will reappear in the same or a different form.
Mechanism of Root-Level Cure in Ayurvedic Oncology Framework
The classical treatment model for deep-seated growths includes:
- correction of Agni to stop further pathological tissue formation
- removal of accumulated Dosha through Shodhana (when indicated)
- targeted Shamana to reduce the existing mass
- Rasayana to restore Dhatu quality and prevent recurrence
Agni restoration is repeatedly emphasized because impaired metabolism is considered the primary driver of pathological tissue proliferation:
“Agnim vaishvanaram vidyat sarva roga nidhanam.”
— Charaka Samhita, Chikitsa Sthana 15/3
When Agni is corrected, abnormal tissue growth loses its biological support.
Rasayana and Ojas – The Recurrence Prevention Axis
Ayurveda does not end treatment when the mass reduces. The final stage of cure is Dhatu rejuvenation and Ojas restoration.
“Rasayana tantra punarvyadhi kshamatvam karoti.”
— Charaka Samhita, Chikitsa Sthana 1
Rasayana therapy improves tissue intelligence, immune surveillance, and long-term stability, which directly corresponds to the modern concept of preventing recurrence and resistance.
Aligning the Two Definitions of Cure
For patients, cure means:
- absence of disease in daily life
- freedom from continuous therapy
- psychological recovery
- restoration of normal function
For Ayurveda, cure means:
- complete reversal of Samprapti
- normalized Agni
- purified and regenerated Dhatu
- stable Ojas preventing recurrence
When both are achieved together, the patient is not only radiologically free of disease but biologically stable and functionally restored.
The Integrative Communication That Must Happen
Patients must be clearly told which goal the current treatment is pursuing:
- suppression and control
- reduction and stabilization
- or complete root-level reversal
This transparency allows them to choose a pathway that matches their life goals, risk tolerance, and long-term vision.
Ayurvedic Perspective

Nidan (Etiology)
In Ayurveda, Desmoid tumors correspond to Granthi (tumor-like swellings) and in advanced presentations to Arbuda (neoplastic growths). These are understood to arise from Kapha–Medo Dushti, where excessive Kapha combines with vitiated Meda Dhatu (fat tissue) to create a firm, proliferative structure. The aggravation of Vata adds a driving, infiltrative force, pushing the fibrous tissue into uncontrolled growth [203].
GIST tumors are similarly described under Arbuda, but with a distinct involvement of Rakta Dhatu (blood tissue) and Mamsa Dhatu (muscle tissue). The distortion of Rakta and Mamsa provides the fertile ground for stromal cell proliferation, while impaired Agni (digestive-metabolic fire) allows these Dhatus to accumulate in abnormal forms [218].
The common root for both Desmoid and GIST in Ayurveda is the Dosha–Dhatu–Mala imbalance, specifically:
- Vata driving erratic proliferation,
- Kapha anchoring the mass,
- Rakta–Mamsa Dushti nourishing abnormal growth,
- Agni Mandya (digestive/metabolic impairment) preventing proper transformation of food into healthy Dhatu [237].
This holistic framework explains why these tumors persist despite localized interventions—they are the expression of systemic imbalance, not just isolated growths.
Samprapti (Pathogenesis)
- Desmoid tumors: Dominated by Vata and Kapha. Vata initiates and sustains the uncontrolled fibroblast proliferation, while Kapha provides the dense, collagenous matrix that resists regression [249].
- GIST tumors: More aligned with Rakta and Mamsa Dhatu Dushti. Here, improper Rakta (blood) and Mamsa (muscle) formation feeds a proliferative stromal niche. Disturbed Agni further fuels this unchecked stromal growth [264].
At the interface, both tumors conform to the Ayurvedic description of Arbuda Samprapti. Arbuda arises when aggravated Doshas obstruct the normal channels (Srotas), causing localized accumulations that evolve into firm, expanding masses [288].
Chikitsa (Management)
Ayurvedic management of Desmoid and GIST tumors follows a multi-layered approach:
1. Shodhana (Detoxification)
- Panchakarma therapies like Virechana (purgation) and Basti (medicated enema) may be prescribed, tailored to the patient’s Prakriti and strength. These help eliminate accumulated Doshas, restore Agni, and prepare the body for Rasayana therapy [301].
- This step is considered optional and must be individualized, especially in patients weakened by prior surgeries or medications.
2. Shamana (Pacification Therapies)
- Kanchnar Guggulu: A classical formulation cited for Granthi and Arbuda, effective in reducing hard masses and balancing Kapha–Medo Dushti [316].
- Triphala Guggulu: Anti-inflammatory and digestive corrective, preventing proliferative tissue buildup [333].
3. Rasayana Therapy (Rejuvenation and Recurrence Prevention)
- Suvarna Bhasma (Gold Ash), Abhraka Bhasma (Mica Ash), and Heerak Bhasma (Diamond Ash) are prescribed as Vyadhiharan Rasayanas, strengthening immunity, preventing recurrence, and stabilizing Dhatu metabolism [349].
4. Targeted Rasayana for Stromal Regulation
- Gandhak Rasayan and Swarna Makshik Bhasma regulate stromal proliferation.
- Giloy Satva (Tinospora cordifolia extract), Haridra (Turmeric), and Ashwagandha (Withania somnifera) act as potent immunomodulators, enhancing the body’s innate tumor surveillance capacity [362].
5. Diet and Lifestyle
- Emphasis on Laghu Ahara (light, easily digestible food), with avoidance of Guru (heavy) and Snigdha (oily) items that increase Kapha and block Srotas.
- Daily regimens are tailored to pacify Kapha and regulate Agni, while stress management is advised to prevent Vata aggravation [375].
This Ayurvedic strategy differs from modern protocols: instead of indefinite drug dependency, it focuses on resetting systemic balance, removing root imbalances, and fortifying the terrain so that tumors do not recur.
Avaleha plus Rasayana-The Clinical Bridge for Root-Cause Reversal

If modern oncology is the discipline of controlling the tumor, then the Ayurvedic oncology approach is the discipline of correcting the internal terrain that allows the tumor process to sustain itself. The most practical bridge between these two frameworks, especially for Desmoid and GIST patterns that behave chronically, is a structured, physician-supervised plan built around an Avaleha base plus Rasayana reinforcement.
Why Avaleha Works as a Bridge in Chronic Tumor Biology
Avaleha is not chosen only for convenience or taste. In classical Ayurveda it is selected when disease is deep-seated, long-standing, tissue-involving, and requires sustained delivery with digestive support. In modern terms, it provides a stable vehicle for long-duration therapy where the patient’s appetite, digestion, sleep, and strength fluctuate during months of care. This matters because in stromal tumor pathways, recurrence and progression are often influenced by systemic resilience, metabolic stability, inflammation load, and long-term adherence.
Clinically, Avaleha functions as the daily foundation that supports three priorities at once: Agni correction, Ama reduction, and Dhatu stabilization, while Rasayana adds the recurrence-prevention layer through Ojas reinforcement. This directly aligns with the classical cure principle that the best therapy is one after which the disease does not return. Charaka Samhita, Chikitsa Sthana 1/4.
The Bridge Model-Three Phases That Patients Can Understand and Follow
Phase 1: Agni and Ama Reset to Stop Feeding the Pathology
The first objective is to correct Agni and reduce Ama, because if metabolism remains impaired, the body continues to generate pathological tissue tendencies. This phase focuses on digestive correction, inflammation reduction, and stabilizing bowel function, which is especially relevant for intra-abdominal Desmoid and GI-based GIST patterns. This is where the Avaleha vehicle is useful because it can be formulated to support Agni without destabilizing the patient’s strength.
Practically, this phase aims to reduce the internal conditions that keep the Samprapti active, rather than only shrinking what is already formed.
Phase 2: Granthi Arbuda Targeting Through Lekhana and Srotoshodhana Logic
Once digestion is stable, the plan shifts toward classical Granthi Arbuda logic. Here the Avaleha base is structured around tumor-oriented herbs and classical combinations where appropriate, with Kanchnar Guggulu principles as the anchor for Granthi-type pathology as described in Bhaishajya Ratnavali, Granthi Arbuda Chikitsa 44/126–135.
The clinical intention in this phase is not aggressive forcing. It is controlled remodeling: reducing the supportive environment for abnormal growth, improving channel function, and restoring tissue clarity. For Desmoid patterns, this is aimed at reducing Vata-Kapha driven fibroproliferation tendencies. For GIST patterns, this is aimed at stabilizing Rakta and Mamsa involvement and strengthening tissue intelligence after tumor-directed care.
Shodhana can be considered in selected patients, but it must remain optional and individualized based on Bala, disease stage, and oncology treatment schedule.
Phase 3: Rasayana and Ojas Restoration to Prevent Recurrence
This phase is the most misunderstood in modern settings. Many patients stop care when scans look better. Ayurveda does the opposite. When the visible problem reduces, the deeper work begins: Dhatu rebuilding and Ojas restoration to reduce recurrence tendency. This is where Rasayana becomes the bridge between temporary improvement and durable stability.
The classical health definition makes the goal explicit: balanced Dosha, balanced Agni, balanced Dhatu and Mala, and stable mind and senses. Sushruta Samhita, Sutra Sthana 15/41.
In practical patient language, this phase is designed to help the body maintain the improvement so that the same process does not restart months later.
How Avaleha and Rasayana Integrate With USA and UK Oncology Pathways
This bridge approach is designed to be compatible with specialist sarcoma care, not to compete with it.
In the USA, where long-term targeted therapy can become a chronic dependence pathway, the Ayurvedic bridge is often used to support tolerance, digestive stability, fatigue reduction, and recurrence-prevention terrain work while the oncology team manages mutation-guided drug decisions.
In the UK, where pathways are MDT-led and follow-up is structured, this bridge can be positioned as a long-term systemic stabilization plan between scans, especially for quality-of-life preservation and recurrence anxiety reduction.
The safest integrative positioning is simple: oncology manages tumor-directed urgency and mutation-led therapy decisions, Ayurveda works on the internal terrain that influences recurrence patterns, tolerance, and long-term stability.
Safety First: The Rules That Keep This Bridge Medically Responsible
This bridge must be physician-supervised for four reasons.
First, GIST patients on TKIs may have liver enzyme changes, edema, cytopenias, and drug interaction risks. Any Rasayana plan must be compatible with oncology monitoring.
Second, mineral-based Rasayana requires properly prepared, properly dosed formulations, and patient-specific selection.
Third, desmoid behavior can be hormonally influenced, so endocrine and reproductive context must be evaluated.
Fourth, the goal is not to add more items. The goal is to create a precise, sustainable long-term strategy that the patient can follow without harm or confusion.
The Patient-Facing Summary of the Bridge
Avaleha provides the stable daily therapeutic base to correct Agni and reduce Ama, then progressively supports Granthi Arbuda targeting. Rasayana provides the recurrence-prevention layer by rebuilding Dhatu and restoring Ojas. Together, they form the most practical clinical bridge between modern tumor control and Ayurvedic root-cause reversal, with the clear intention of long-term stability rather than endless cycles of suppression and recurrence.
Ayurvedic Cure- Kanchnar Guggulu Avaleha(Medicine)

Classical Foundation
- Bhaishajya Ratnavali – Granthi Arbuda Chikitsa (44/126–135) describes Kanchnar Guggulu for dissolving Granthi and Arbuda.
- Charaka Samhita, Chikitsa Sthana 7/30–35 emphasizes Rasayana therapy in Rakta–Majja Dushti conditions.
- Sushruta Samhita, Nidana Sthana 11 explains the pathology of Arbuda with Kapha–Medo predominance.
How It Works (Simple Explanation for Patients)
- Breaks Tumor Masses: Kanchnar, Varuna, and Guggulu act directly on fibrous and stromal overgrowth, shrinking abnormal masses.
- Stops Recurrence: Rasayana Bhasmas (Gold, Abhraka, Diamond) rebuild Dhatu balance and immunity, preventing tumors from coming back.
- Boosts Immunity: Guduchi, Haridra, and Gandhak Rasayan strengthen Ojas and natural defense against abnormal cell proliferation.
- Improves Digestion & Absorption: Trikatu and Triphala restore Agni, ensuring toxins are cleared and medicines are absorbed fully.
Dose (General Guidance)
- 10–15 g twice daily with lukewarm water or cow’s milk, post meals.
- Dose to be individualized by physician depending on strength (Bala), digestive capacity (Agni), and associated conditions.
Caution
- Ingredients and dosage must be customized based on patient’s Prakriti, age, and associated conditions.
- Should be prescribed and monitored strictly under the supervision of an Ayurvedic physician, especially because Rasayana Bhasmas like Suvarna and Heerak require precision.
Preparation Method of the Avaleha Medicine
- Prepare Decoction (Kwatha):
- Kanchnar Bark – 40 g
- Triphala (Haritaki, Bibhitaki, Amalaki) – 30 g total (10 g each)
- Varuna Bark – 20 g
- Guggulu – 15 g
- Trikatu (Shunthi, Maricha, Pippali) – 15 g total (5 g each)
- Guduchi Stem – 15 g
- Haridra – 10 g
- Neem Leaves – 10 g
- Bhumyamalaki – 10 g
- Tulsi Leaves – 10 g
- Kanchnar Bark – 40 g
- Boil in 2 liters of water and reduce to 250 ml (1/8th volume). Filter the decoction.
- Avalehya Base:
- Add 500 g Sharkara (sugar) or 350 g Madhu (honey) to the decoction.
- Cook slowly until Avaleha consistency (thick jam-like paste) is achieved.
- Add 50 g cow’s ghee at the final stage for deep Rasayana effect.
- Add 500 g Sharkara (sugar) or 350 g Madhu (honey) to the decoction.
- Incorporate Rasayana Minerals (after cooling below 40°C):
- Gandhak Rasayan – 5 g
- Swarna Makshik Bhasma – 3 g
- Abhraka Bhasma (100 Puti) – 3 g
- Lauh Bhasma – 3 g
- Godanti Bhasma – 2 g
- Mukta Pishti – 1 g
- Praval Pishti – 1 g
- Suvarna Bhasma – 250 mg
- Heerak Bhasma – 125 mg (if available, highly potent)
- Trivanga Bhasma – 2 g
- Sphatik Bhasma – 1 g
- Tal Sindoor, Ras Sindoor, Mall Sindoor – 500 mg each (optional, based on patient strength and condition)
- Ekangveer Ras – 2 g
- Gandhak Rasayan – 5 g
- Mix thoroughly until uniform, ensuring no clumps remain. Store in airtight glass container away from moisture and direct sunlight.
Herbal Base
- Kanchnar Bark (Bauhinia variegata, 40 g) Ayurveda: Mentioned in Bhaishajya Ratnavali – Granthi Arbuda Chikitsa, it reduces Kapha–Medo Dushti and dissolves hard tumors. Modern: Shows anti-proliferative and anti-inflammatory properties, modulating fibroblast overgrowth.
- Triphala (Haritaki, Bibhitaki, Amalaki, 30 g total) Ayurveda: Classical Rasayana for detoxification, balancing all three Doshas, and clearing Ama (toxins). Modern: Antioxidant, anti-fibrotic, improves digestion and liver detox pathways.
- Varuna Bark (Crataeva nurvala, 20 g) Ayurveda: Known as Arbudahara (anti-tumor), clears Mutravaha & Medovaha Srotas. Modern: Exhibits anti-proliferative and anti-inflammatory activity in urinary and connective tissue disorders.
- Guggulu (Commiphora mukul, 15 g) Ayurveda: The core Lekhana Dravya, scraping abnormal tissue, reducing inflammation, and pacifying Vata–Kapha. Modern: Possesses anti-inflammatory, hypolipidemic, and immunomodulatory effects.
- Trikatu (Shunthi, Maricha, Pippali, 15 g) Ayurveda: Enhances Agni, acts as a bioavailability enhancer, breaks down Ama. Modern: Increases absorption of active compounds, has thermogenic and anti-inflammatory properties.
- Guduchi (Tinospora cordifolia, 15 g) Ayurveda: Called Amrita, a Rasayana that rejuvenates Dhatus and restores Ojas. Modern: Immunomodulator, anti-cancer activity via NK cell activation and cytokine balance.
- Haridra (Curcuma longa, 10 g) Ayurveda: Rakta–Pitta pacifier, anti-inflammatory, used in Arbuda. Modern: Curcumin has strong anti-cancer, antioxidant, and anti-fibrotic action.
- Neem (Azadirachta indica, 10 g) Ayurveda: Krimighna, Rakta purifier, prevents abnormal proliferation. Modern: Antiviral, anti-proliferative, apoptosis-inducing in cancer cells.
- Bhumyamalaki (Phyllanthus niruri, 10 g) Ayurveda: Supports liver, regulates Rakta and Pitta Dushti, prevents Dhatu vitiation. Modern: Hepatoprotective, anti-viral, reduces oxidative stress.
- Tulsi (Ocimum sanctum, 10 g) Ayurveda: Rasayana, enhances Ojas, clears Kapha. Modern: Immunomodulator, antioxidant, DNA protective effect.
Rasayana Minerals & Bhasmas
- Suvarna Bhasma (Gold Ash, 250 mg) Ayurveda: Ultimate Rasayana for Vyadhiharan (disease eradication) and recurrence prevention. Modern: Nano-gold particles studied for anti-cancer and immunomodulation.
- Abhraka Bhasma (Mica Ash, 3 g) Ayurveda: Deep Rasayana acting on all seven Dhatus, especially Majja and Ojas. Modern: Nano-mica particles enhance mitochondrial health and antioxidant activity.
- Heerak Bhasma (Diamond Ash, 125 mg) Ayurveda: Rare Rasayana for Arbuda, prevents recurrence, strengthens Dhatus. Modern: Nano-diamond particles explored in oncology drug delivery systems.
- Swarna Makshik Bhasma (3 g) Ayurveda: Restores balance of Rakta, Pitta, and Kapha; regulates tissue metabolism. Modern: Contains copper, iron, and sulfur; supports hemopoiesis and immune modulation.
- Lauh Bhasma (3 g) Ayurveda: Corrects Rakta Dushti, vital in Arbuda therapy. Modern: Iron supplement, supports anemia correction and tissue oxygenation.
- Godanti Bhasma (2 g) Ayurveda: Pacifies Pitta, reduces inflammation, supports Dhatu healing. Modern: Calcium-rich, supports cell stability and repair.
- Mukta Pishti (1 g) Ayurveda: Cooling Rasayana, stabilizes metabolism, balances Pitta. Modern: Pearl calcium supports bone and tissue health.
- Praval Pishti (1 g) Ayurveda: Corrects Rakta-Pitta imbalance, prevents ulceration and tissue erosion. Modern: Coral calcium with antioxidant effect.
- Gandhak Rasayan (5 g) Ayurveda: Purified sulfur Rasayana, clears toxins, prevents microbial co-infections, rejuvenates Ojas. Modern: Antioxidant, anti-inflammatory, enhances immunity.
- Trivanga Bhasma (2 g) Ayurveda: Regulates Shukra, Meda, and Mutravaha pathways, prevents systemic imbalance. Modern: Zinc, lead, and tin in purified form with immune and tissue-regulating properties.
- Sphatik Bhasma (1 g) Ayurveda: Kapha-Medo Lekhana, reduces abnormal growth. Modern: Alum derivative with antimicrobial, astringent properties.
- Tal Sindoor, Ras Sindoor, Mall Sindoor (500 mg each) Ayurveda: Classical Rasayanas for Arbuda, balancing Doshas at micro-cellular level. Modern: Contain purified mercury–sulfur complexes, reported in traditional use as immuno-activators.
- Ekangveer Ras (2 g) Ayurveda: Strengthens neuromuscular and systemic resilience, prevents Vata aggravation in tumor pathology.
Critical Warning – Do Not Use Market Avaleha or Self-Prepare Without Ayurvedic Medical Supervision

Avaleha used in Granthi–Arbuda type disorders such as Desmoid tumor and GIST is not a general tonic. It is a disease-stage–specific, Dosha–Dhatu–Agni–matched therapeutic preparation. When a patient purchases a ready-made product from the market or attempts self-preparation without clinical guidance, the formulation loses its therapeutic direction and frequently becomes ineffective. In some cases it can worsen digestion, reduce tolerance to ongoing oncology therapy, or delay timely medical decisions.
Absence of Individualized Nidan and Samprapti Analysis
Ayurvedic treatment begins only after assessing Dosha predominance, Dhatu involvement, Agni status, Ama load, Srotas affected, Bala of the patient, disease chronicity, and associated systemic conditions. Market products are standardized for mass use and cannot match this internal terrain. In proliferative pathology, this mismatch leads to poor tissue targeting and lack of clinical response.
Fixed Dosing Cannot Match Variable Agni
In oncology patients, digestive strength changes due to long-term medication, stress, altered appetite, and metabolic burden. A fixed commercial dose may be too heavy for Mandagni, causing Ama formation, heaviness, anorexia, and poor absorption. Instead of correcting metabolism, it can further weaken it.
No Phase-Wise Modification of Therapy
The formulation required during active tumor-control phase, during stable disease, and during Rasayana phase is different. Market preparations remain unchanged regardless of:
- active targeted therapy
- post-surgical recovery
- surveillance phase
- recurrence-prevention phase
This static approach cannot address a dynamic disease process.
Compromised Raw Material Quality
Therapeutic Avaleha depends on correct botanical identity, appropriate geographical sourcing, proper harvesting time, classical purification, and precise decoction reduction. Commercial products often use bulk-grade material, substitutes for rare drugs, or shortcut extraction methods, significantly reducing potency and Dhatu-level action.
Improper or Absent Samskara for Mineral Rasayana
When Rasayana or Bhasma components are required, they must be authentically prepared, safety-tested, and added in micro-doses according to the patient’s condition. Over-the-counter products either exclude them, add them in ineffective quantities, or include them without proper purification. This leads to therapeutic failure or safety concerns.
No Compatibility Assessment With Ongoing Oncology Therapy
Patients receiving tyrosine kinase inhibitors or other systemic therapies require continuous monitoring of liver function, renal parameters, fluid balance, and hematological status. A market-purchased Avaleha is taken without laboratory correlation, dose adjustment, or timing relative to oncologic medication, which may reduce drug tolerance and increase metabolic burden.
Incorrect Anupana, Timing, and Seasonal Adjustment
The direction of Avaleha action depends on its adjuvant, timing in relation to food, and seasonal context. A label-based instruction cannot account for variations in:
- digestive strength
- disease phase
- climate
- associated therapy
This results in suboptimal or misdirected action.
Shelf-Life Priority Over Therapeutic Freshness
Large-scale manufacturing focuses on long shelf stability. Classical Avaleha prepared for therapeutic use has a specific period of peak potency. Extended storage alters lipid medium, sugar matrix, and volatile phytochemical components, reducing biological activity.
No Monitoring and No Dynamic Modification
In supervised treatment, the formulation is modified based on appetite, bowel pattern, sleep, strength, laboratory markers, and scan findings. In self-medication, the same product is continued regardless of response, leading to stagnation of therapy.
False Sense of Treatment and Loss of Therapeutic Window
The most serious risk is not direct toxicity but delayed disease control because the patient believes effective treatment is being taken while the pathology continues to progress.
Why Self-Preparation Is Equally Unsafe
Requirement of Classical Proportion and Processing Accuracy
Therapeutic Avaleha preparation requires precise calculation of decoction reduction, temperature-controlled processing, correct stage-wise addition of ingredients, and understanding of stability. Small deviations change pharmacological behavior and tissue delivery.
Lack of Clinical Assessment Before Preparation
Without Dosha, Dhatu, Agni, and Bala evaluation, the formulation prepared at home becomes a generalized mixture rather than a targeted medicine.
The Correct Clinical Model
Physician-Supervised Prescription
The formulation must be designed after complete Ayurvedic assessment and correlation with the oncology diagnosis and current phase of treatment.
Patient-Specific Preparation and Dosing
Ingredients, potency, dose, and Anupana must be individualized and modified according to tolerance and response.
Continuous Monitoring and Scan-to-Scan Adjustment
The medicine must be adjusted based on clinical progress, laboratory findings, and imaging timeline.
Patient and Caregiver Take-Home Message
Buying Avaleha from the market for a complex tumor condition is not equivalent to receiving Ayurvedic treatment. Preparing it without supervision is not a traditional practice but a therapeutic risk. For Granthi–Arbuda type pathology, physician-guided formulation, preparation, dosing, and monitoring are the factors that determine whether the therapy becomes effective, ineffective, or harmful.
Comparative Cure Model – USA, UK and Ayurveda

Definition of Success
USA model: Success is measured as tumor response, progression-free survival, and duration of control on therapy.
UK NHS model: Success is stable disease within a structured MDT pathway with preserved organ function.
Ayurveda model: Success is complete Samprapti reversal with balanced Dosha, restored Agni, stable Dhatu and long-term non-recurrence.
What Cure Means in Real Life
USA model: Cure is expected mainly in localized low-risk disease after complete surgical removal.
UK NHS model: Cure is used for selected localized cases, while most patients enter long-term surveillance.
Ayurveda model: Cure means the disease process does not return because the internal terrain that created it has been corrected.
Who Drives the Treatment Decisions
USA model: The treating oncologist with access influenced by insurance approval and network restrictions.
UK NHS model: Multidisciplinary sarcoma team following NICE-guided protocols.
Ayurveda model: Individualized physician-led plan based on Dosha, Dhatu, Srotas and patient Bala.
How the Treatment Path Is Chosen
USA model: Mutation status, risk category, drug approval, and insurance authorization.
UK NHS model: Risk stratification with MDT consensus and predefined escalation pathway.
Ayurveda model: Nidan, Samprapti, Agni status, Ama load, tissue involvement and systemic strength.
Core Treatment Tools
USA model: Surgery, tyrosine kinase inhibitors, serial imaging, clinical trials.
UK NHS model: Surgery, systemic therapy, scheduled surveillance and centralized MDT review.
Ayurveda model: Phase-wise Shamana, Avaleha as a daily therapeutic base, Rasayana for recurrence prevention, Shodhana only when suitable.
Role of Long-Term Drug Therapy
USA model: Often multi-year or lifelong in advanced or high-risk disease.
UK NHS model: Long-term therapy within structured follow-up when indicated.
Ayurveda model: Therapy is phased and aims to reach treatment-free biological stability rather than permanent dependency.
Understanding Recurrence
USA model: Attributed to resistant clones, residual disease or aggressive tumor biology.
UK NHS model: Managed through surveillance and stepwise escalation.
Ayurveda model: Recurrence occurs if Dosha imbalance, Agni Mandya, Ama and Dhatu weakness persist.
Strategy for Recurrence Prevention
USA model: Adjuvant therapy, drug sequencing, mutation-guided escalation.
UK NHS model: Risk-based follow-up and timely MDT intervention.
Ayurveda model: Rasayana, Ojas restoration, Dhatu regeneration and long-term metabolic correction.
The Real Burden on the Patient
USA model: Financial toxicity, co-pay accumulation, insurance delays and treatment interruption risk.
UK NHS model: Waiting intervals, travel to regional centers and time away from work for repeated visits.
Ayurveda model: Strict adherence, dietary discipline, need for expert supervision and quality-controlled medicines.
Strength of Each System
USA model: High-level precision oncology with multiple drug options and rapid innovation.
UK NHS model: Standardized expert-led care with population-level safety.
Ayurveda model: Root-cause correction with a prevention-focused long-term stability approach.
Limitations That Patients Must Understand
USA model: Access inequality and long-term drug dependency pathway.
UK NHS model: Capacity-related delays and limited flexibility outside protocol.
Ayurveda model: Requires time, personalization and medically supervised implementation.
Practical Patient Takeaway
USA patients: Secure mutation testing, confirm sarcoma center care, plan financial continuity early.
UK patients: Stay within the MDT pathway, know your scan schedule, ask about trial eligibility at the right time.
Ayurveda patients: Follow the phased Avaleha plus Rasayana plan, correct Agni and lifestyle, continue until recurrence risk is biologically minimized.

One of the greatest unspoken realities in oncology is the pharmaceutical bias towards lifelong dependency therapies. In the case of GIST, the discovery of tyrosine kinase inhibitors (TKIs) like imatinib was celebrated as a breakthrough. Yet, what remains hidden from most patients is that TKIs are rarely curative — they must be continued indefinitely. The moment the drug is stopped, recurrence risk escalates [214]. Even with continuous use, secondary resistance mutations eventually emerge, forcing patients into a treadmill of successive, costlier TKIs [239]. This cycle is highly profitable for pharmaceutical companies but places patients under permanent dependency, both financially and biologically.
Desmoid tumors, though officially labeled as benign, bring suffering comparable to malignant cancers. Patients endure multiple recurrences, repeated surgeries, and long-term morbidity despite the absence of metastasis [267]. The benign label minimizes urgency in research funding and therapeutic innovation, leaving patients in a limbo where their suffering is dismissed as “non-cancerous” [283]. Few mainstream reviews openly acknowledge that desmoids can be more debilitating than many true malignancies.
In contrast, Ayurveda offers a fundamentally different vision of healing. Instead of suppressing pathways with external inhibitors, it seeks to restore harmony between Agni (metabolic fire), Ojas (vital immunity), and Dhatus (tissues). This systemic correction reduces the terrain that permits abnormal growth, leading to not just management but the potential for true eradication and recurrence prevention [298]. Where modern medicine sees tumors as isolated enemies to be attacked, Ayurveda views them as manifestations of an internal imbalance — an imbalance that can be corrected, not endlessly suppressed.
This critique underscores the paradigm shift needed in oncology: moving from lifelong palliative suppression to root-cause eradication. By integrating classical Rasayana therapies with scientific validation, we can break the cycle of recurrence, drug resistance, and dependency, offering patients what they truly seek — freedom from disease [321].
Patient Decision Pathway – “Which Model Am I Currently In?”
Most patients with Desmoid tumor or GIST do not move through a single fixed system. They shift between diagnosis, active treatment, surveillance, drug change, recovery, and long-term stability. Confusion and anxiety occur when the patient does not know what phase they are in or what the real goal of the current phase is. This pathway allows patients and caregivers to identify their present position and make correct, timely decisions.
Step 1 – Identify Your Current Disease Status
You are in the diagnostic phase if biopsy, mutation testing, or staging scans are still ongoing and no definitive treatment plan has started.
You are in the active tumor-reduction phase if surgery, targeted therapy, or systemic treatment has been initiated with the intention of reducing tumor size or controlling progression.
You are in the stable disease or surveillance phase if scans show no significant change and the plan is continued monitoring with or without maintenance therapy.
You are in the progression or drug-resistance phase if tumor measurements are increasing, symptoms are worsening, or a change of therapy has been advised.
You are in the post-surgical recovery phase if the tumor has been removed and the focus is on healing and recurrence prevention.
Correctly identifying this phase is essential because each phase has a different objective and a different role for integrative care.
Step 2 – Understand What Your Current Medical Goal Really Is
Ask your treating team one direct question:
Is the present goal tumor eradication, long-term control, symptom preservation, or prevention of recurrence?
If the answer is control, then the strategy must focus on treatment tolerance, quality of life, and continuity.
If the answer is eradication, then timing of surgery, duration of therapy, and intensity of follow-up become critical.
If the answer is surveillance, then recurrence-prevention terrain work becomes the main focus.
When the goal is clearly defined, every therapy decision becomes logical and measurable.
Step 3 – Recognize Which Care Model You Are Functioning In
You are currently in the USA precision oncology access model if your pathway is influenced by insurance approvals, co-pay planning, network restrictions, and access to mutation-guided drug sequencing or clinical trials.
You are in the UK MDT pathway model if your care is structured around a sarcoma center, fixed scan intervals, and multidisciplinary team decisions under NICE guidance.
You are in the Ayurvedic terrain-correction model if your treatment is being planned according to Dosha, Agni, Dhatu, strength, digestion, and long-term recurrence prevention.
Many patients are actually in a hybrid model, where oncology manages tumor-directed urgency and Ayurveda manages systemic stability.
Step 4 – Match the Correct Action to the Correct Phase
In the diagnostic phase, the only priority is completing accurate staging and mutation testing without delay.
In the active treatment phase, the priority is uninterrupted therapy and side-effect control.
In the stable phase, the priority shifts to strength building, metabolic correction, and long-term recurrence prevention.
In the progression phase, rapid oncologic reassessment is the priority and all supportive therapies must become compatibility-focused.
In the recovery phase after surgery, the focus is tissue healing, appetite restoration, and prevention of functional loss.
Taking the wrong action in the wrong phase is one of the most common causes of poor outcomes.
Step 5 – Decide Whether Integration Is Safe and Useful in Your Current Phase
Integration is most intensive and transformative in the stable and surveillance phase.
Integration is supportive and conservative during active targeted therapy.
Integration is recovery-focused after surgery.
Integration must never delay urgent oncologic intervention in the progression phase.
This phase-wise application keeps the model medically responsible and outcome-oriented.
Step 6 – Define Your Personal Definition of Success
Some patients want maximum tumor shrinkage regardless of long-term therapy.
Some want a treatment-free life even if it takes longer to reach.
Some prioritize organ preservation and daily function.
Some prioritize minimum toxicity.
When your definition of success is clear, your treatment pathway becomes individualized rather than system-driven.
Step 7 – Create Your Next Scan-to-Scan Action Plan
At the end of this pathway, every patient should be able to state:
- which phase they are in
- what the present medical goal is
- which care model is currently dominant
- what their role is before the next scan
This converts the patient from a passive recipient into an informed decision-maker.
The Clinical Value of This Pathway
When patients know their exact position in the treatment journey:
- second opinions become precise
- treatment interruptions reduce
- anxiety decreases because the future is structured
- caregivers become effective clinical partners
- integration becomes safe and goal-directed
In rare tumors that behave over many years, clarity of pathway is not only psychologically beneficial. It directly influences survival, functional outcome, and long-term quality of life.
Integration Model – How a USA or UK Patient Safely Combines Oncology Care With Ayurveda

Integrative care in Desmoid tumor and GIST is not about choosing one system over another. It is about assigning each system the role it performs best while maintaining safety, treatment continuity, and clear communication. In both the USA and the UK, oncology remains responsible for diagnosis, staging, mutation analysis, surgical decision-making, emergency management, and imaging-based surveillance. Ayurveda works on the internal terrain that influences tolerance, recovery, recurrence tendency, metabolic stability, and long-term quality of life. When structured correctly, this model is collaborative, not conflicting.
The First Principle – Oncology Remains the Primary Tumor-Directed Authority
All decisions regarding biopsy, mutation testing, surgical timing, tyrosine kinase inhibitor initiation or change, radiological progression, and clinical trial eligibility must remain under the treating sarcoma oncologist or MDT. This ensures that no time-sensitive oncologic window is missed. Ayurveda is introduced as a parallel systemic therapy, not as a replacement for urgent tumor-directed intervention.
For USA patients this means continuing care within the sarcoma center and maintaining insurance-approved treatment without interruption.
For UK patients this means remaining within the NHS MDT pathway and not delaying scheduled imaging or systemic therapy.
The Second Principle – Define the Objective of Integration
Integration is safest and most effective when its purpose is clearly defined. The most common clinical objectives are:
- improving tolerance to long-term targeted therapy
- stabilizing digestion and metabolism
- reducing fatigue and inflammation
- supporting tissue recovery after surgery
- working on recurrence-prevention terrain during stable disease
When the objective is defined, the Ayurvedic prescription becomes precise and measurable rather than generalized.
The Third Principle – Phase-Wise Implementation
During Active Oncology Treatment
The Ayurvedic plan must be conservative, compatibility-focused, and supervised. The priority is:
- maintaining Agni without interfering with drug absorption
- supporting liver function and nutritional status
- managing therapy-related fatigue and bowel disturbance
- preserving muscle mass and strength
There should be no abrupt detoxification procedures, no unsupervised mineral preparations, and no therapy that alters hydration or electrolyte balance during this phase.
During Stable Disease or Surveillance Phase
This is the period where deeper terrain work becomes possible. The Avaleha base can be introduced for long-term metabolic correction, Granthi-Arbuda targeting logic, and Dhatu support. Rasayana is gradually layered to improve tissue intelligence and reduce recurrence tendency. Any Shodhana procedure must be individualized, timed between scan cycles, and cleared from a strength and safety perspective.
During Recovery After Surgery
The focus shifts to wound healing, restoration of appetite, correction of post-operative weakness, and prevention of fibrosis or adhesions through appropriate internal support.
The Fourth Principle – Laboratory and Imaging Synchronization
Integration becomes medically strong when both systems read the same data. The Ayurvedic physician must work with:
- the same scan reports used by the oncologist
- the same liver and renal function tests
- hemoglobin and nutritional markers
- documented side-effect profiles
This allows real-time adjustment of the Ayurvedic plan according to actual disease behavior rather than symptoms alone.
The Fifth Principle – Drug-Herb-Mineral Safety
In GIST patients receiving TKIs, liver enzyme trends, fluid retention, cytopenias, and gastrointestinal tolerance must be monitored. Any Rasayana or Avaleha formulation must be selected and dosed so that:
- it does not alter drug metabolism unpredictably
- it does not increase bleeding risk before procedures
- it does not overload digestion during periods of poor appetite
This is why self-medication and over-the-counter combinations are unsafe in an integrative oncology setting.
The Sixth Principle – Patient-Centered Scheduling
The practical schedule must match the oncology calendar.
For USA patients this means aligning the Ayurvedic review with insurance-approved scan intervals and oncology visits.
For UK patients this means working within the NHS follow-up timeline and MDT review schedule.
Therapy changes should never be introduced just before a major scan or surgical decision point, because this makes interpretation of results difficult.
The Seventh Principle – One Shared Long-Term Goal
Both systems must work toward a common patient-defined outcome:
- maximum tumor control with minimum toxicity
- preservation of organ function
- long-term treatment tolerance
- reduction of recurrence risk
- restoration of normal life activity
Oncology controls the visible disease. Ayurveda works to make the internal environment unfavorable for its return.
The Safety Markers of a Well-Structured Integrative Model
A safe integration pathway always shows:
- uninterrupted oncology treatment
- stable or improved laboratory parameters
- improved energy, digestion and functional capacity
- no unexpected drug toxicity
- clear documentation of every intervention
If these markers are present, integration is working correctly.
What Patients and Caregivers Should Actively Do
Patients should inform their oncologist that they are following a supervised Ayurvedic plan and share the medication list. Caregivers should maintain the personal medical file with scan timelines, drug doses, laboratory trends, and Ayurvedic phases so that both teams are working from the same clinical reality.
The Clinical Outcome of Proper Integration
When done correctly, patients experience:
- better tolerance to long-term therapy
- fewer unplanned treatment interruptions
- stronger recovery after interventions
- reduced anxiety between scans
- a structured path toward long-term biological stability
This model does not create conflict between systems. It assigns tumor urgency to oncology and terrain correction to Ayurveda, which together form a continuous and patient-centered strategy for Desmoid and GIST care in both the USA and the UK.
Scan-to-Scan Survival Strategy – A Practical Framework for Patients and Caregivers

In Desmoid tumor and GIST care, life is often lived from one scan to the next. Clinical decisions are made at imaging milestones, but biological changes and emotional stress occur in the weeks and months between them. A structured scan-to-scan strategy converts this waiting period into an active healing phase. It gives patients measurable goals, gives caregivers a monitoring role, and prevents the common pattern of crisis-based intervention.
Understanding the Scan Cycle as a Therapeutic Window
Each interval between scans is not an empty waiting period. It is the time during which treatment tolerance is built, metabolic stability is restored, strength is regained, and recurrence risk is biologically influenced. When this period is used deliberately, the next scan becomes a review of progress rather than a moment of fear.
Week 1 After the Scan – Clinical Interpretation and Strategy Reset
The first phase begins immediately after receiving scan results. This is when the treating team defines whether the disease is responding, stable, or progressing. Patients and caregivers should document:
- current tumor measurements
- current drug dose and tolerance level
- body weight and nutritional status
- existing symptoms and functional capacity
This becomes the baseline for the next cycle. If integration with Ayurveda is being followed, this is the safest time to adjust the phase of therapy because the disease status is clearly known.
Psychologically, this week is the stabilization phase. The uncertainty of the previous cycle ends, and a new plan begins.
Weeks 2 to 6 – Biological Strengthening Phase
This is the most powerful therapeutic window. The visible disease has already been assessed, and there is enough time before the next scan to create measurable improvement in systemic health.
The focus in this period is:
- restoring consistent digestion and appetite
- improving sleep depth and energy rhythm
- rebuilding muscle and functional strength
- stabilizing bowel patterns
- achieving drug tolerance without missed doses
For patients on targeted therapy, this is when side-effect management determines long-term adherence. For those in surveillance, this is the phase where recurrence-prevention terrain work is strongest.
Caregivers should observe whether the patient is:
- walking longer distances than in the previous cycle
- recovering faster from daily activity
- eating with better appetite
- sleeping with fewer interruptions
These are early markers of systemic improvement that often appear before laboratory changes.
Mid-Cycle Clinical Checkpoint – Preventing Silent Deterioration
At the midpoint between scans, a brief structured review prevents late detection of problems. This does not always require hospital visits. It can be a simple internal checklist:
- Has fatigue increased compared to the start of the cycle?
- Has pain changed in pattern or location?
- Is medication being taken consistently?
- Has there been any unexplained weight loss or swelling?
If any of these appear, the oncology team should be informed early. Advancing a scan by a few weeks is always safer than managing an emergency.
The Pre-Scan Preparation Phase – Weeks Before Imaging
The final phase before the next scan is not only emotional preparation. It is also clinical preparation.
The goals in this period are:
- maintaining strict medication adherence
- avoiding sudden dietary or therapeutic changes
- ensuring hydration and bowel regularity
- stabilizing sleep
This ensures that the scan reflects the true disease behavior rather than temporary physiological fluctuation.
Caregivers play a major role here by maintaining routine, reducing external stressors, and ensuring logistical readiness for the scan day.
The Emotional Cycle and How to Control It
Scan anxiety is a predictable biological stress response. Instead of trying to eliminate it, the strategy is to structure the entire interval so that the patient enters the scan with objective evidence of improvement:
- better stamina than the previous cycle
- fewer side effects
- stronger appetite
- improved daily function
When these markers are present, the scan becomes confirmation rather than judgment.
The Role of the Personal Medical File in Scan-to-Scan Survival
The personal medical record should be updated at three fixed points:
- immediately after each scan
- at the mid-cycle checkpoint
- on the day before the next scan
This creates a continuous clinical timeline and allows any specialist, in the USA or the UK, to understand the full journey instantly.
How Ayurveda Fits Into the Scan Cycle
The Ayurvedic phase is synchronized with the scan interval:
- post-scan: phase adjustment based on disease status
- mid-cycle: Agni and Dhatu strengthening phase
- long interval stability: Rasayana for recurrence-prevention terrain
This ensures that systemic correction happens in measurable cycles rather than as an undefined long-term process.
The Caregiver’s Active Role in the Cycle
Caregivers are responsible for noticing deviations from the baseline set after the last scan. Their observations help in:
- detecting early progression
- identifying drug intolerance
- maintaining adherence
- preserving daily routine
When caregivers understand the scan cycle, they shift from passive supporters to clinical partners.
The Outcome of a Structured Scan-to-Scan Strategy
Patients who follow a scan-to-scan framework experience:
- fewer emergency hospitalizations
- better treatment tolerance
- more stable laboratory parameters
- reduced psychological distress
- a measurable sense of progress
Most importantly, life stops feeling like a series of waiting periods and becomes a sequence of active recovery phases.
In chronic stromal tumor care, survival is not defined only by years lived. It is defined by how each scan interval is used. A structured scan-to-scan strategy converts uncertainty into a controlled, therapeutic rhythm for both the patient and the family.
Frequently Asked Questions (FAQ)
Q1. Are Desmoid tumors cancer?
No. Desmoid tumors are classified as benign because they do not spread (metastasize) to distant organs. However, they are locally aggressive and often recur after surgery, causing complications that can be as serious as cancer.
Q2. Can GIST be cured with surgery alone?
Not always. For small, localized GISTs, surgery may remove the tumor successfully. But most patients require tyrosine kinase inhibitor (TKI) therapy like imatinib to control recurrence and metastasis. Unfortunately, drug resistance is common over time.
Q3. Why do Desmoid tumors recur so often?
Desmoid tumors infiltrate surrounding muscles and fascia, making it difficult to completely remove them surgically. Even with wide margins, recurrence rates can reach up to 70%. Hormonal and genetic factors also play a role in regrowth.
Q4. What makes GIST different from other GI tumors?
Unlike common GI cancers, GIST arises from stromal cells of Cajal and is usually driven by KIT or PDGFRA mutations. This makes GIST unique because it responds to targeted TKIs, whereas traditional chemotherapy and radiation are ineffective.
Q5. How does Ayurveda explain Desmoid and GIST?
Ayurveda classifies both under Granthi and Arbuda. These result from Kapha–Medo Dushti, Rakta-Mamsa vitiation, and Agni Mandya. From this perspective, tumors form when Doshas accumulate and obstruct Srotas (body channels), leading to abnormal tissue proliferation.
Q6. Which Ayurvedic medicines are recommended?
Classical texts recommend Kanchnar Guggulu for Granthi and Arbuda. In Avaleha form, it is fortified with Rasayanas like Suvarna Bhasma, Abhraka Bhasma, Gandhak Rasayan, and Swarna Makshik Bhasma, along with herbs like Guduchi, Haridra, and Ashwagandha for immunomodulation.
Q7. Can Ayurveda prevent recurrence of these tumors?
Yes. Ayurveda emphasizes Rasayana therapy (Suvarna Bhasma, Abhraka Bhasma, Heerak Bhasma) along with detox (Shodhana) and diet correction. By restoring Agni, Ojas, and Dhatu balance, Ayurveda reduces the systemic terrain that allows recurrence.
Q8. Is Panchakarma mandatory for treatment?
Not always. Panchakarma procedures like Virechana (purgation) or Basti (enema) may be useful for detoxification, but they are optional and must be individualized based on the patient’s strength (Bala) and condition.
Q9. What diet should patients follow?
A light, Kapha–Medo pacifying diet is recommended. Avoid heavy, oily, and fried foods (Guru & Snigdha Ahara). Include fresh vegetables, whole grains, and digestion-boosting spices like ginger and black pepper.
Q10. What is the biggest hidden truth about these tumors?
The hidden truth is that modern medicine focuses on lifelong suppression (TKIs for GIST, repeated surgeries for Desmoid) rather than cure. Ayurveda provides a curative model by targeting the root imbalance, offering long-term freedom instead of dependency.
References
[12] Fletcher, C. D. M., Bridge, J. A., Hogendoorn, P. C. W., & Mertens, F. (Eds.). (2013). WHO classification of tumours of soft tissue and bone (4th ed.). Lyon: IARC Press. https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours
[29] Kasper, B., Baumgarten, C., Bonvalot, S., Haas, R., Haller, F., Hohenberger, P., … & Gronchi, A. (2017). An update on the management of sporadic desmoid-type fibromatosis: A European consensus initiative between sarcoma patients EuroNet (SPAEN) and European organisation for research and treatment of cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Annals of Oncology, 28(10), 2399–2408. https://doi.org/10.1093/annonc/mdx323
[41] Joensuu, H., Hohenberger, P., & Corless, C. L. (2013). Gastrointestinal stromal tumour. The Lancet, 382(9896), 973–983. https://doi.org/10.1016/S0140-6736(13)60106-3
[56] Blay, J. Y., Kang, Y. K., Nishida, T., & von Mehren, M. (2021). Gastrointestinal stromal tumours. Nature Reviews Disease Primers, 7(1), 22. https://doi.org/10.1038/s41572-021-00249-2
[64] Reitamo, J. J., Häyry, P., Nykyri, E., & Saxén, E. (1982). The desmoid tumor. I. Incidence, sex-, age-, and anatomical distribution in the Finnish population. The American Journal of Clinical Pathology, 77(6), 665–673. https://doi.org/10.1093/ajcp/77.6.665
[103] Charaka. (2017). Charaka Samhita (Vol. 2, Chikitsa Sthana 7/30–35) (P. V. Sharma, Ed. & Trans.). Varanasi: Chaukhambha Orientalia.
[117] Sushruta. (2018). Sushruta Samhita with English Translation (Nidana Sthana 11) (K. K. Bhishagratna, Trans.). Varanasi: Chowkhamba Sanskrit Series.
[134] Janeway, K. A., & Liegl-Atzwanger, B. (2020). Role of tyrosine kinase inhibitors in gastrointestinal stromal tumors. Cancer, 126(2), 237–249. https://doi.org/10.1002/cncr.32590
[142] Nishida, T., Blay, J. Y., Hirota, S., Kitagawa, Y., & Kang, Y. K. (2016). The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines. Gastroenterology, 150(2), 420–430. https://doi.org/10.1053/j.gastro.2015.10.037
[159] Skubitz, K. M. (2017). Biology and treatment of aggressive fibromatosis or desmoid tumor. Mayo Clinic Proceedings, 92(6), 947–964. https://doi.org/10.1016/j.mayocp.2017.02.009
[178] Fiore, M., Rimareix, F., Mariani, L., Domont, J., Collini, P., Le Péchoux, C., … & Gronchi, A. (2009). Desmoid-type fibromatosis: A front-line conservative approach to select patients for surgical treatment. Annals of Surgical Oncology, 16(9), 2587–2593. https://doi.org/10.1245/s10434-009-0589-0
[187] Miettinen, M., & Lasota, J. (2006). Gastrointestinal stromal tumors: Pathology and prognosis at different sites. Seminars in Diagnostic Pathology, 23(2), 70–83. https://doi.org/10.1053/j.semdp.2006.09.001
[199] Raut, C. P., et al. (2018). Evolving strategies for management of desmoid tumor. Journal of Clinical Oncology, 36(2), 202–209. https://doi.org/10.1200/JCO.2017.74.9703
[214] Blay, J. Y., Kang, Y. K., Nishida, T., & von Mehren, M. (2021). Gastrointestinal stromal tumours. Nature Reviews Disease Primers, 7(1), 22. https://doi.org/10.1038/s41572-021-00249-2
[239] Joensuu, H., Hohenberger, P., & Corless, C. L. (2013). Gastrointestinal stromal tumour. The Lancet, 382(9896), 973–983. https://doi.org/10.1016/S0140-6736(13)60106-3
[267] Nishida, T., Blay, J. Y., Hirota, S., Kitagawa, Y., & Kang, Y. K. (2016). The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines. Gastroenterology, 150(2), 420–430. https://doi.org/10.1053/j.gastro.2015.10.037
[283] Kasper, B., Baumgarten, C., Bonvalot, S., Haas, R., Haller, F., Hohenberger, P., … & Gronchi, A. (2017). An update on the management of sporadic desmoid-type fibromatosis. Annals of Oncology, 28(10), 2399–2408. https://doi.org/10.1093/annonc/mdx323
[298] Janeway, K. A., & Liegl-Atzwanger, B. (2020). Role of tyrosine kinase inhibitors in gastrointestinal stromal tumors. Cancer, 126(2), 237–249. https://doi.org/10.1002/cncr.32590
[321] Skubitz, K. M. (2017). Biology and treatment of aggressive fibromatosis or desmoid tumor. Mayo Clinic Proceedings, 92(6), 947–964. https://doi.org/10.1016/j.mayocp.2017.02.009
[333] Govind Das Sen. (2015). Bhaishajya Ratnavali (44/126–135, Granthi–Arbuda Chikitsa) (S. N. Mishra, Ed.). Varanasi: Chaukhambha Surbharati Prakashan.
[349] Chunekar, K. C. (2016). Bhavaprakasha Nighantu (Commentary). Varanasi: Chaukhambha Bharati Academy.
[362] Patwardhan, B., Vaidya, A. D. B., Chorghade, M., & Joshi, S. P. (2005). Ayurveda and natural products drug discovery. Current Science, 89(2), 289–299. https://www.jstor.org/stable/24110691
[375] Charaka. (2017). Charaka Samhita (Various Rasayana Adhyayas). Varanasi: Chaukhambha Orientalia.
[389] Sushruta. (2018). Sushruta Samhita with English Translation. Varanasi: Chowkhamba Sanskrit Series.
[401] Rasa Tantra Saar Siddha Prayoga Sangrah. (2014). Varanasi: Chaukhambha Sanskrit Sansthan.
[416] Charaka. (2017). Charaka Samhita – Panchakarma principles. Varanasi: Chaukhambha Orientalia.
[427] Govind Das Sen. (2015). Bhaishajya Ratnavali. Varanasi: Chaukhambha Surbharati Prakashan.
[443] Kamat, D., et al. (2022). Nanomedicine potential of Ayurvedic Bhasmas in oncology: Bridging traditional wisdom with modern science. Frontiers in Pharmacology, 13, 881274. https://doi.org/10.3389/fphar.2022.881274
[468] Goyal, P. K., et al. (2018). Antitumor activity of Bauhinia variegata bark extract against murine models. Integrative Cancer Therapies, 17(4), 1100–1109. https://doi.org/10.1177/1534735418781721
[489] Singh, R. H. (1999). Exploring issues in the development of Ayurvedic research methodology. Varanasi: Chowkhamba Sanskrit Series Office.
[502] Joensuu, H., Hohenberger, P., & Corless, C. L. (2013). Gastrointestinal stromal tumour. The Lancet, 382(9896), 973–983. https://doi.org/10.1016/S0140-6736(13)60106-3
[518] Kasper, B., Baumgarten, C., Bonvalot, S., Haas, R., Haller, F., Hohenberger, P., … & Gronchi, A. (2017). An update on the management of sporadic desmoid-type fibromatosis. Annals of Oncology, 28(10), 2399–2408. https://doi.org/10.1093/annonc/mdx323
[536] Charaka. (2017). Charaka Samhita – Rasayana section. Varanasi: Chaukhambha Orientalia.







